GLP-1 Booster Supplements: What the Evidence Actually Shows
Abstract / Summary
This comprehensive guide examines supplements marketed as "GLP-1 boosters," revealing the gap between marketing claims and scientific evidence. While some compounds like berberine have legitimate metabolic effects, they work primarily through non-GLP-1 mechanisms (AMPK activation) and produce modest results (2-3 pounds weight loss over 12 weeks) compared to pharmaceutical GLP-1 agonists (15% body weight reduction). The article provides evidence-based analysis of individual compounds, explains how marketing exploits technical accuracy to create misleading impressions, and positions supplements appropriately within metabolic health hierarchy.
GLP-1 Booster Supplements: What the Evidence Actually Shows
Do GLP-1 booster supplements actually work? If you’ve been scrolling through social media or browsing supplement aisles lately, you’ve probably encountered products claiming to “naturally boost GLP-1” or provide “GLP-1 support without a prescription.” These supplements emerged alongside the explosive popularity of prescription GLP-1 medications like Ozempic and Wegovy, positioning themselves as accessible alternatives for weight management and metabolic health.
The marketing narrative is compelling: achieve similar benefits through natural compounds like berberine, chromium, or proprietary herbal blends—without injections, prescriptions, or insurance battles. But when supplement companies claim their products “boost GLP-1 levels” or “support GLP-1 activity,” what does that actually mean? And more importantly, does the evidence support these claims?
This article examines the science behind supplements marketed as GLP-1 booster supplements. You’ll learn what GLP-1 actually does in your body, which compounds have research backing, what the studies actually show (versus what marketing implies), and how to evaluate these products critically. We’re not here to sell you supplements or dismiss them categorically—we’re here to help you understand what the evidence actually demonstrates.
Scope note: This article focuses exclusively on dietary supplements and natural compounds marketed for GLP-1 effects. It does not cover prescription GLP-1 receptor agonists like semaglutide (Ozempic, Wegovy) or tirzepatide (Mounjaro), which work through entirely different mechanisms and have substantially more clinical evidence.
To understand what “GLP-1 booster” claims actually mean, we first need to establish what GLP-1 does in the body—and why this became such an attractive marketing angle for supplements.
Section 2: Understanding GLP-1 Physiology
Before evaluating supplement claims, you need to understand what GLP-1 actually does—and why it became central to metabolic health discussions.
What Is GLP-1?
Glucagon-like peptide-1 (GLP-1) is an incretin hormone secreted by specialized L-cells in your intestinal lining. When you eat, these cells release GLP-1 into your bloodstream, triggering a cascade of metabolic effects that help regulate blood sugar and energy balance 1Drucker, D.J. “The biology of incretin hormones.” Cell Metabolism, 2006; 3(3): 153-165..
Think of GLP-1 as a coordination signal: it tells your pancreas to release insulin, signals your brain that you’re satisfied, and slows digestion to prevent blood sugar spikes. It’s not a single-purpose hormone—it orchestrates multiple systems simultaneously.
The Multiple Functions of GLP-1
Glucose Regulation GLP-1 stimulates insulin secretion from pancreatic beta cells, but only when blood glucose is elevated—a crucial safety feature that prevents dangerous low blood sugar 2Holst, J.J. “The physiology of glucagon-like peptide 1.” Physiological Reviews, 2007; 87(4): 1409-1439.. Simultaneously, it suppresses glucagon release, reducing the liver’s glucose output when it’s not needed.
Appetite and Satiety Control GLP-1 slows gastric emptying, meaning food stays in your stomach longer, extending the physical sensation of fullness. More significantly, it acts directly on appetite centers in the hypothalamus, reducing hunger signals and food-seeking behavior 3Müller, T.D. et al. “Glucagon-like peptide 1 (GLP-1).” Molecular Metabolism, 2019; 30: 72-130.. This central nervous system effect is why GLP-1 influences eating behavior beyond just mechanical stomach fullness.
Beyond Metabolism: Emerging Research Recent studies suggest GLP-1 may have cardiovascular protective effects and potential neuroprotective properties, though these areas remain under active investigation 4Nauck, M.A. et al. “Cardiovascular actions and clinical outcomes with glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors.” Circulation, 2017; 136(9): 849-870.. The hormone’s effects extend well beyond simple appetite control.
Why GLP-1 Became Relevant to Weight Management
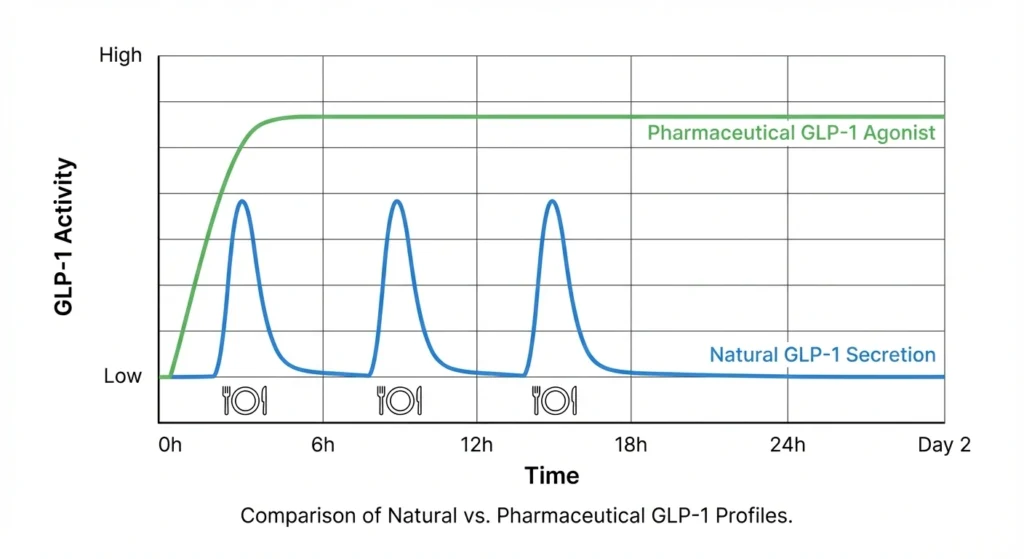
Natural GLP-1 secretion creates transient satiety—the satisfied feeling after a meal that gradually fades as the hormone is broken down. Your body produces GLP-1 in response to eating, but an enzyme called dipeptidyl peptidase-4 (DPP-4) rapidly degrades it, giving natural GLP-1 a half-life of only 1-2 minutes 5Deacon, C.F. “Physiology and pharmacology of DPP-4 in glucose homeostasis and the treatment of type 2 diabetes.” Frontiers in Endocrinology, 2019; 10: 80..
This is where pharmaceutical GLP-1 receptor agonists changed the game. Medications like semaglutide (Ozempic, Wegovy) are modified to resist DPP-4 breakdown, maintaining high GLP-1 activity for days rather than minutes. This sustained activation produces continuous appetite suppression and metabolic effects that natural, meal-triggered GLP-1 secretion cannot match.
The Critical Distinction for Supplement Evaluation
Natural GLP-1 secretion:
- Triggered by meals, rises and falls within hours
- Rapidly degraded by DPP-4 enzyme (1-2 minute half-life)
- Transient receptor activation
- Physiological concentrations
Pharmaceutical GLP-1 agonists:
- Continuous presence regardless of eating
- Engineered DPP-4 resistance (days-long activity)
- Sustained receptor activation
- Supraphysiological concentrations
This difference is fundamental to understanding supplement claims. When a product promises to “boost GLP-1,” the relevant question isn’t just whether it increases GLP-1 secretion temporarily—it’s whether that increase produces meaningful, sustained metabolic effects comparable to what makes pharmaceutical agonists effective.
With this understanding of GLP-1’s role in metabolism and the distinction between transient secretion and sustained activation, we can now evaluate what GLP-1 booster supplements actually contain—and whether they deliver on their marketing promises.
Section 3: The GLP-1 Booster Supplement Category
Walk into any supplement store or browse online retailers, and you’ll find dozens of products labeled as “GLP-1 boosters,” “GLP-1 support,” or “natural GLP-1 activators.” But what exactly are these supplements, and what does this category actually represent?
What’s Being Sold as GLP-1 Booster supplements
The “GLP-1 booster” label encompasses a diverse collection of compounds, most commonly:
Berberine – A plant alkaloid that has become the flagship ingredient in GLP-1 supplement marketing, often positioned as “nature’s Ozempic”
Fiber supplements – Glucomannan, psyllium husk, and other soluble fibers that slow digestion and potentially trigger incretin release
Minerals – Chromium picolinate and other trace minerals linked to glucose metabolism
Antioxidants – Alpha-lipoic acid, resveratrol, and similar compounds with metabolic effects
Plant extracts – Green tea, cinnamon, bitter melon, and various traditional medicine ingredients
These compounds are frequently combined into proprietary blends with names that emphasize their GLP-1 connection. The dosages in commercial formulations often fall below the amounts used in research studies—a detail marketing materials rarely highlight.
The Marketing Framework
“GLP-1 booster” is a marketing category, not a scientific classification. The labeling strategy follows a predictable pattern:
Association with pharmaceutical success – Products are positioned alongside or as alternatives to prescription GLP-1 medications, implying comparable mechanisms and results.
Selective study citation – Marketing highlights research showing that specific compounds can increase GLP-1 secretion, while omitting context about magnitude, duration, or clinical significance.
Mechanism emphasis over outcomes – Product descriptions focus on “naturally boosting GLP-1 production” rather than demonstrating that this boost produces meaningful metabolic effects.
“Natural alternative” positioning – The framing suggests you can achieve prescription-like results through “natural” supplementation, without acknowledging the fundamental differences in GLP-1 activity levels and duration.
The Questions That Matter
The marketing framework obscures three critical distinctions:
- Can these supplements increase GLP-1 secretion? Some can, modestly and transiently.
- Does that increase produce effects comparable to pharmaceutical GLP-1 agonists? No—the magnitude and duration of GLP-1 elevation differ dramatically.
- Do these supplements have metabolic benefits through other mechanisms? This is the more relevant question, which we’ll address in the next section.
Understanding the Category’s Limitations
“GLP-1 booster” conflates multiple compounds with different mechanisms under a single umbrella term. Berberine works differently than fiber supplements, which work differently than chromium—yet all are marketed with similar GLP-1-focused claims.
The evidence base varies substantially between compounds. Some have robust research demonstrating metabolic benefits (though not through sustained GLP-1 elevation). Others have minimal evidence beyond preliminary cell studies or animal research. The category label obscures these important distinctions.
Whether any particular supplement proves useful depends on the specific compound, dosage, quality of the product, and your individual metabolic context—not on whether it carries a “GLP-1 booster” label.
To understand what these supplements actually do—beyond marketing claims—we need to examine the individual compounds and their evidence bases.
Section 4: Individual Compound Analysis
To evaluate GLP-1 booster supplements effectively, we need to examine the evidence for individual compounds—what they actually do, what the research demonstrates, and how marketing claims diverge from scientific reality.
Berberine: The Most Evidence, The Most Overstated
Berberine has become the flagship ingredient in GLP-1 supplement marketing, frequently labeled “nature’s Ozempic.” This positioning is both the most understandable and the most misleading in the category.
What Berberine Actually Is
Berberine is an isoquinoline alkaloid extracted from various plants in the Berberis family, including goldenseal and barberry. It has extensive use in traditional Chinese and Ayurvedic medicine for gastrointestinal and metabolic conditions 6Yin, J. et al. “Efficacy of berberine in patients with type 2 diabetes mellitus.” Metabolism, 2008; 57(5): 712-717.. Unlike single-target pharmaceuticals, berberine affects multiple molecular pathways simultaneously—which makes it pharmacologically interesting but difficult to characterize simply.
Primary Mechanisms: AMPK, Not GLP-1
Berberine’s dominant metabolic effect comes through activating AMP-activated protein kinase (AMPK), an enzyme that functions as a cellular energy sensor 7Lee, Y.S. et al. “Berberine, a natural plant product, activates AMP-activated protein kinase with beneficial metabolic effects in diabetic and insulin-resistant states.” Diabetes, 2006; 55(8): 2256-2264.. This is the same pathway activated by metformin, the first-line diabetes medication. AMPK activation:
- Enhances glucose uptake into muscle and fat cells
- Improves insulin sensitivity
- Reduces glucose production in the liver
- Influences lipid metabolism
Berberine also modulates gut microbiome composition, which may contribute to its metabolic effects through mechanisms still being elucidated 8Zhang, X. et al. “Structural changes of gut microbiota during berberine-mediated prevention of obesity and insulin resistance in high-fat diet-fed rats.” PLoS One, 2012; 7(8): e42529..
Does berberine increase GLP-1 secretion? Yes, some studies show modest increases 9Yu, Y. et al. “Berberine may rescue Fusobacterium nucleatum-induced colorectal tumorigenesis by modulating the tumor microenvironment.” Oncotarget, 2015; 6(31): 32013-32026.. But this is a minor contributor to its metabolic effects, not the primary mechanism. The “GLP-1 booster” label emphasizes the least important aspect of how berberine works.
What the Evidence Actually Shows
Multiple meta-analyses demonstrate that berberine produces modest but consistent metabolic improvements:
Glucose control: Reductions in fasting blood glucose (averaging 15-25 mg/dL) and HbA1c (0.5-0.7%) in people with type 2 diabetes or prediabetes 10Lan, J. et al. “Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipemia and hypertension.” Journal of Ethnopharmacology, 2015; 161: 69-81..
Insulin sensitivity: Improvements in HOMA-IR (a measure of insulin resistance) comparable to metformin in some studies 11Yin, J. et al. “Efficacy of berberine in patients with type 2 diabetes mellitus.” Metabolism, 2008; 57(5): 712-717..
Weight effects: Meta-analyses show average weight loss of 1-3 pounds over 12 weeks—statistically significant but clinically modest 12Ye, Y. et al. “Efficacy and safety of berberine alone for several metabolic disorders: A systematic review and meta-analysis of randomized clinical trials.” Frontiers in Pharmacology, 2021; 12: 653887..
Lipid profile: Small improvements in LDL cholesterol, triglycerides, and HDL cholesterol.
These are legitimate benefits. They’re also nowhere near pharmaceutical GLP-1 agonist effects. People taking semaglutide lose an average of 15% of body weight over 68 weeks 13Wilding, J.P. et al. “Once-weekly semaglutide in adults with overweight or obesity.” New England Journal of Medicine, 2021; 384(11): 989-1002.. Berberine studies show 2-3% weight loss over similar periods.
Critical Distinctions for Consumers
Berberine has the strongest evidence base among compounds marketed as GLP-1 booster supplements, with consistent research supporting modest improvements in glucose metabolism and insulin sensitivity. However, its primary mechanism is AMPK activation—similar to metformin—rather than GLP-1 manipulation. While some studies show berberine can increase GLP-1 secretion, this is a minor contributor to its metabolic effects.
Calling berberine “nature’s Ozempic” fundamentally misrepresents both what it does and the magnitude of its effects. It’s more accurately described as “nature’s metformin”—and even that comparison overstates the similarity.
Legitimate Use Cases
Berberine may be useful for:
- Metabolic syndrome support (alongside lifestyle changes)
- Prediabetes management
- Modest cardiovascular risk factor modification
- Part of a comprehensive approach to metabolic health
Effective dosing typically requires 500mg taken 2-3 times daily with meals—total daily doses of 1,000-1,500mg. Lower doses common in proprietary blends may not provide meaningful benefits.
What Berberine Is Not
- A weight loss drug replacement
- Comparable to pharmaceutical GLP-1 agonists in mechanism or magnitude
- Effective for everyone (response varies considerably)
- A substitute for dietary and lifestyle modification
Fiber Supplements: Legitimate Benefits, Transient GLP-1 Effects
Soluble fiber supplements represent perhaps the most honest entry in the “GLP-1 booster” category—they genuinely increase GLP-1 secretion, though not in ways that justify pharmaceutical comparisons.
Common Types and Mechanisms
Glucomannan (konjac root), psyllium husk, inulin, and beta-glucan from oats are the most common fiber supplements marketed for metabolic effects. Their mechanisms involve both direct physical effects and indirect hormonal signaling:
GLP-1 secretion: When fiber reaches the colon, gut bacteria ferment it into short-chain fatty acids (SCFAs) like butyrate, propionate, and acetate. These SCFAs stimulate L-cells to secrete GLP-1 14Tolhurst, G. et al. “Short-chain fatty acids stimulate glucagon-like peptide-1 secretion via the G-protein-coupled receptor FFAR2.” Diabetes, 2012; 61(2): 364-371..
Physical satiety: Soluble fiber absorbs water and expands in the stomach, creating physical fullness. It also slows gastric emptying, extending the satiety period after meals 15Clark, M.J. and Slavin, J.L. “The effect of fiber on satiety and food intake: a systematic review.” Journal of the American College of Nutrition, 2013; 32(3): 200-211..
Microbiome support: Prebiotic fibers feed beneficial gut bacteria, influencing metabolic signaling through multiple pathways beyond GLP-1.
What the Evidence Shows
Yes, fiber increases GLP-1 secretion—this is well-established 16Delzenne, N.M. et al. “Targeting gut microbiota in obesity: effects of prebiotics and probiotics.” Nature Reviews Endocrinology, 2011; 7(11): 639-646.. The effect is transient and meal-dependent, rising after fiber consumption and declining as fermentation completes. This is fundamentally different from sustained pharmaceutical GLP-1 elevation.
Meta-analyses on fiber supplementation for weight loss show modest effects: approximately 2-3 pounds over several months 17Thompson, S.V. et al. “Effects of isolated soluble fiber supplementation on body weight, glycemia, and insulinemia in adults with overweight and obesity: a systematic review and meta-analysis of randomized controlled trials.” American Journal of Clinical Nutrition, 2017; 106(6): 1514-1528.. These benefits appear to come primarily through satiety and calorie displacement rather than hormonal manipulation.
Realistic Positioning
Fiber supplements are excellent for overall health—supporting gut microbiome diversity, improving cardiovascular markers, and enhancing satiety. They’re not a weight loss intervention on their own. The GLP-1 increase they produce is a byproduct of healthy digestion, not a pharmaceutical mechanism.
Fiber should be a dietary staple regardless of GLP-1 marketing. The fact that supplements are positioned as “GLP-1 boosters” doesn’t change their fundamental role in a healthy diet—it just adds misleading context to a legitimately beneficial practice.
Other Common Ingredients: Weak Evidence, Strong Marketing
Several other compounds appear regularly in GLP-1 supplement formulations, typically with minimal evidence for the specific claims made:
Chromium Picolinate
Marketed for insulin sensitivity and glucose metabolism, chromium shows weak and inconsistent evidence. Some studies demonstrate small improvements in glucose control; many show no effect 18Balk, E.M. et al. “Effect of chromium supplementation on glucose metabolism and lipids: a systematic review of randomized controlled trials.” Diabetes Care, 2007; 30(8): 2154-2163.. The supplement may help individuals with true chromium deficiency, but most people in developed countries are not deficient. The GLP-1 connection is essentially nonexistent.
Alpha-Lipoic Acid (ALA)
ALA has some legitimate evidence for diabetic neuropathy and functions as an antioxidant 19Ziegler, D. et al. “Treatment of symptomatic diabetic peripheral neuropathy with the anti-oxidant alpha-lipoic acid.” Diabetes Care, 1995; 18(8): 1160-1167.. Effects on glucose metabolism and weight are minimal and inconsistent. Any GLP-1 connection is indirect at best. It’s a legitimate supplement for specific uses—just not the ones emphasized in GLP-1 marketing.
Green Tea Extract (EGCG)
Green tea catechins, particularly EGCG, show very modest thermogenic effects in research. Meta-analyses demonstrate statistically significant but clinically insignificant weight loss—typically less than 2 pounds over months 20Jurgens, T.M. et al. “Green tea for weight loss and weight maintenance in overweight or obese adults.” Cochrane Database of Systematic Reviews, 2012; 12: CD008650.. There is no established GLP-1 connection. Green tea is a healthy beverage choice; the supplement effects are overstated.
Cinnamon Extract
Some studies show small improvements in fasting glucose with cinnamon supplementation; others show no effect 21Allen, R.W. et al. “Cinnamon use in type 2 diabetes: an updated systematic review and meta-analysis.” Annals of Family Medicine, 2013; 11(5): 452-459.. The evidence is inconsistent and effects, when present, are modest. The GLP-1 connection has minimal supporting evidence. Cinnamon is a pleasant culinary spice that may have some metabolic benefits—it’s not a supplement priority.
Bitter Melon
Traditional use in various cultures for blood sugar control hasn’t translated to strong modern evidence. Studies in humans are limited, poorly designed, and show inconsistent results 22Ooi, C.P. et al. “Bitter melon (Momordica charantia) for type 2 diabetes mellitus.” Cochrane Database of Systematic Reviews, 2010; 2: CD007845.. Any GLP-1 connection is speculative. It may have some glucose effects worthy of further research, but current evidence doesn’t support supplementation recommendations.
The Pattern Across Ingredients
These compounds share a common characteristic: they have some metabolic research (allowing technically accurate marketing claims), but effects are small, inconsistent, or poorly replicated in quality studies. The GLP-1 connection is typically absent or misrepresented. They’re often included in proprietary blends at doses below those used in research studies showing even modest effects.
Understanding what these individual compounds do—and more importantly, what they don’t do—reveals the fundamental problem with “GLP-1 booster” marketing: the disconnect between what the science shows and what consumers are led to believe.
Section 5: The Marketing Problem – What “Increases GLP-1” Actually Means
The most sophisticated aspect of “GLP-1 booster supplements” marketing isn’t that it lies—it’s that it tells technically accurate truths in misleading contexts. Understanding this distinction is essential for evaluating supplement claims critically.
The Magnitude Problem: Not All Increases Are Equal
When a supplement company claims their product “boosts GLP-1,” they’re often making a technically defensible statement. Some compounds do increase GLP-1 secretion measurably. The problem is what that claim doesn’t tell you.
Research shows that compounds like berberine or fiber can increase GLP-1 levels by 10-30% above baseline 23Yu, Y. et al. “The therapeutic effects of berberine in cardiovascular disease, gastrointestinal disease and endocrine disease.” Frontiers in Pharmacology, 2021; 12: 658163.. This sounds significant until you understand the context: baseline GLP-1 secretion is transient and rapidly degraded, with a circulating half-life of 1-2 minutes due to DPP-4 enzyme activity 24Deacon, C.F. “Physiology and pharmacology of DPP-4 in glucose homeostasis and the treatment of type 2 diabetes.” Frontiers in Endocrinology, 2019; 10: 80..
A 30% increase in something that disappears in minutes is fundamentally different from pharmaceutical GLP-1 agonists, which maintain therapeutic concentrations continuously for days. It’s the difference between turning up a dimmer switch slightly and installing stadium floodlights.
Transient Spikes vs. Sustained Activation
Natural GLP-1 secretion—including supplement-enhanced secretion—follows a predictable pattern: it rises after meals as food triggers L-cell release, peaks within 30-60 minutes, and returns to baseline as DPP-4 degrades the hormone. This creates brief windows of GLP-1 activity that coincide with eating.
Pharmaceutical GLP-1 receptor agonists like semaglutide are engineered to resist DPP-4 breakdown, maintaining high receptor activation 24 hours a day 25Lau, J. et al. “Discovery of the once-weekly glucagon-like peptide-1 (GLP-1) analogue semaglutide.” Journal of Medicinal Chemistry, 2015; 58(18): 7370-7380.. This continuous signaling produces effects that episodic, supplement-induced increases cannot replicate.
The biological significance isn’t just about the peak level—it’s about sustained receptor occupancy. Brief GLP-1 spikes may not produce the same metabolic reprogramming as continuous activation, regardless of how high those spikes reach.
Borrowed Credibility and Association Bias
“GLP-1 booster supplement” marketing exploits the massive success of prescription GLP-1 medications by creating association without equivalence. Products are positioned near pharmaceutical brand names in marketing materials, using phrases like “natural GLP-1 support” or “works on the same pathway as [prescription drug].”
These associations are technically accurate—many compounds do affect GLP-1 secretion pathways—but they create false equivalencies. They allow consumers to mentally link supplement outcomes with pharmaceutical outcomes, even though the mechanisms differ fundamentally in duration, magnitude, and biological effect.
This borrowed credibility transforms modest metabolic benefits into expectations of dramatic weight loss, leveraging pharmaceutical success to sell unrelated products.
How Marketing Exploits Scientific Language
Cherry-picking studies: Marketing materials cite research demonstrating GLP-1 increases while omitting discussion of effect sizes, duration, or clinical outcomes. A study showing berberine increases GLP-1 by 20% becomes “clinically proven to boost GLP-1” without contextualizing what that means.
Mechanism emphasis over outcomes: By focusing on the pathway (“activates GLP-1 production”) rather than the result (“produces 2-3 pound weight loss over 12 weeks”), marketing allows consumers to assume pharmaceutical-level outcomes from pathway similarity.
Selective endpoint reporting: Studies showing any positive metabolic effect—improved insulin sensitivity, modest glucose reductions—become evidence that the supplement “works,” even when the measured outcome differs entirely from what consumers expect based on pharmaceutical comparisons.
Association without attribution: Phrases like “supports the GLP-1 pathway” or “promotes healthy GLP-1 levels” are scientifically meaningless but marketing gold—they imply pharmaceutical mechanisms without making specific, falsifiable claims.
What “Boosts GLP-1” Doesn’t Tell You
When you see a “GLP-1 booster” claim, ask four questions the marketing won’t answer:
- How much? (Magnitude of increase)
- For how long? (Duration of elevation)
- With what effect? (Biological significance)
- Compared to what? (Pharmaceutical vs. natural baseline context)
Saying a supplement “boosts GLP-1” is like saying a candle “increases illumination.” Technically true, but the relevant question is: by how much, and is it enough to accomplish what you need? A candle increases illumination in a dark room, but it’s not a replacement for stadium floodlights. Similarly, some supplements increase GLP-1 secretion, but they don’t produce pharmaceutical-level concentrations or sustained metabolic effects.
Marketing sophistication lies in stating accurate facts while encouraging inaccurate conclusions. The supplement increases GLP-1 (true). GLP-1 is the mechanism behind successful weight loss drugs (true). Therefore, the supplement produces similar effects (false, but never explicitly stated).
Despite these marketing limitations, this doesn’t mean GLP-1 booster supplements are worthless. Understanding who might actually benefit—and with what realistic expectations—requires a more nuanced assessment.
Section 6: Who Might Benefit (With Realistic Expectations)
Not everyone who purchases “GLP-1 booster” supplements will be wasting their money—but success requires appropriate expectations, realistic goals, and understanding when these supplements might offer genuine value versus when they’re unlikely to help.
Potential Candidates for Metabolic Support Supplements
Metabolic Syndrome and Prediabetes Support
Individuals with metabolic syndrome—defined as having at least three of the following: elevated waist circumference, high triglycerides, low HDL cholesterol, elevated blood pressure, or impaired fasting glucose 26Grundy, S.M. et al. “Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement.” Circulation, 2005; 112(17): 2735-2752.—represent the most evidence-based use case for supplements like berberine.
Research consistently shows berberine producing modest improvements in fasting glucose (15-25 mg/dL reductions), HbA1c (0.5-0.7% decreases), and lipid markers in people with insulin resistance or prediabetes 27Lan, J. et al. “Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipemia and hypertension.” Journal of Ethnopharmacology, 2015; 161: 69-81.. These effects are meaningful for metabolic optimization when combined with lifestyle modifications—they’re not dramatic weight loss interventions.
Realistic expectation: Small but measurable improvements in glucose and lipid markers over 2-3 months. Weight effects will be modest (2-3 pounds maximum). This is supplementary support alongside diet and exercise changes, not a replacement for them.
General Metabolic Health Optimization
Health-conscious individuals already implementing solid nutrition and exercise habits might use these supplements for marginal metabolic gains. This represents using supplements for their actual evidence-based effects rather than for marketing-promised outcomes.
Berberine for modest insulin sensitivity improvements, fiber for satiety support and microbiome benefits, or specific compounds for targeted metabolic effects can provide small advantages when expectations align with reality.
Realistic expectation: Minor supportive role as part of a comprehensive health strategy. Measurable benefits on glucose monitors or lipid panels, not dramatic body composition changes. You’re optimizing already-good metabolic health, not correcting metabolic dysfunction.
Fiber and Gut Health Focus
Anyone seeking to increase dietary fiber intake—for gut microbiome diversity, cardiovascular benefits, or satiety support—can benefit from fiber supplements regardless of GLP-1 marketing. The fact that fiber increases GLP-1 transiently is interesting physiologically but not the primary reason to consume it.
Glucomannan, psyllium, inulin, and other prebiotic fibers support general health through multiple mechanisms 28Holscher, H.D. “Dietary fiber and prebiotics and the gastrointestinal microbiota.” Gut Microbes, 2017; 8(2): 172-184.. Marketing them as “GLP-1 boosters” doesn’t diminish their actual benefits—it just adds misleading context.
Realistic expectation: Improved satiety, better digestive regularity, potential modest cardiovascular benefits. Not pharmaceutical-level weight loss or appetite suppression.
Who Will Likely Be Disappointed
People Seeking Pharmaceutical-Level Weight Loss
If your goal is 10-20% body weight reduction, Ozempic-comparable appetite suppression, or dramatic metabolic transformation without lifestyle changes, “GLP-1 booster” supplements will disappoint. The magnitude and mechanism simply don’t support these expectations.
Marketing creates this mismatch intentionally—associating supplements with pharmaceutical success to drive sales to consumers who need pharmaceutical interventions. Supplements showing 2-3 pound weight loss over 12 weeks cannot replace medications producing 15-20% body weight reductions.
Those Needing Medical Intervention
Clinical obesity (BMI ≥30 or ≥27 with comorbidities), type 2 diabetes requiring management, or other metabolic conditions needing pharmaceutical treatment should not be addressed primarily through supplements marketed with misleading GLP-1 claims.
The risk here isn’t just wasted money—it’s delayed effective treatment. Time spent trying ineffective supplements instead of pursuing evidence-based medical care can allow conditions to progress unnecessarily.
Metabolically Healthy Individuals
If your glucose metabolism, insulin sensitivity, and weight are already optimal, adding “GLP-1 booster” supplements provides minimal benefit. You’re attempting to optimize a system that’s already functioning well, which rarely produces meaningful results.
Preventive supplementation makes sense when evidence supports specific benefits for healthy populations. For most compounds in “GLP-1 booster” products, that evidence doesn’t exist.
Integration Strategy for Those Who Proceed
If you decide these supplements align with your health strategy, approach them systematically:
Foundation First Establish solid nutrition, consistent exercise, adequate sleep, and stress management before adding supplements. These compounds work best as support for good habits, not replacements for absent ones.
Evidence-Based Selection Focus on compounds with actual research backing: berberine at 1,000-1,500mg daily, fiber supplements at effective doses (5-10g), or specific ingredients with demonstrated benefits for your particular metabolic concerns. Avoid proprietary blends with under-dosed ingredients.
Outcome Monitoring Track measurable markers: fasting glucose, HbA1c, lipid panels, body weight. If you see no improvements after 3 months, discontinue. Don’t continue based on marketing promises rather than actual results.
Quality Considerations Choose products with third-party testing certifications verifying ingredient identity, purity, and absence of contaminants. For detailed guidance on evaluating supplement quality and understanding third-party testing certifications, see our supplement certifications comparison guide.
Medical Coordination Berberine can interact with medications, particularly diabetes drugs, potentially causing excessive blood sugar lowering when combined with metformin or other glucose-lowering agents 29Yin, J. et al. “Efficacy of berberine in patients with type 2 diabetes mellitus.” Metabolism, 2008; 57(5): 712-717.. If you take prescription medications or have managed medical conditions, inform your healthcare provider about supplement use.
For those who decide these supplements might fit their health strategy, understanding how to evaluate products and avoid deceptive marketing is essential.
Section 7: Evaluating GLP-1 Booster Products
If you’ve decided a metabolic support supplement aligns with your health strategy, distinguishing legitimate products from marketing-heavy formulations requires systematic evaluation. Here’s how to approach product selection critically.
Red Flags in Marketing Claims
Pharmaceutical Comparisons Any product positioning itself as “nature’s Ozempic,” claiming to “work like prescription medications,” or promising “same results without a prescription” is fundamentally misrepresenting what supplements can accomplish. These comparisons exploit pharmaceutical success to sell unrelated products with different mechanisms and magnitudes of effect.
Similarly, “doctor-developed” or “clinically formulated” claims without specific study citations are credibility signals without substance. Legitimate research involvement requires identifying the actual studies, not just asserting professional development.
Unrealistic Weight Loss Promises Specific guarantees like “lose 20 pounds in 30 days” or claims that results require “no diet or exercise” contradict the evidence base for these compounds. Meta-analyses show berberine producing 2-3 pound weight loss over 12 weeks in best-case scenarios 30Ye, Y. et al. “Efficacy and safety of berberine alone for several metabolic disorders: A systematic review and meta-analysis of randomized clinical trials.” Frontiers in Pharmacology, 2021; 12: 653887.—not dramatic rapid weight reduction.
Marketing emphasizing “automatic fat melting” or similar passive weight loss mechanisms indicates the product is being sold on fantasy rather than evidence.
Proprietary Blend Obfuscation “Proprietary GLP-1 boosting complex” or similar language typically hides inadequate ingredient dosing. When a product lists “Proprietary Blend: 500mg” containing five ingredients without individual amounts, you cannot verify whether any compound reaches research-supported doses.
Claims of “clinically studied formulas” mean nothing without identifying the actual studies. Legitimate research citations include author names, publication years, and journal names—not vague references to unnamed “clinical trials.”
Testimonial Over Evidence Products emphasizing before/after photos, celebrity endorsements, or “as seen on TV” claims over scientific evidence are selling transformation narratives rather than evidence-based metabolic support. Unverifiable customer testimonials are marketing, not data.
Pressure and Scarcity Tactics “Limited time breakthrough,” “secret formula,” artificial stock scarcity, or fear-based messaging about “missing the opportunity” are sales tactics, not quality indicators. Legitimate products don’t require urgency manufacturing to drive purchases.
Evidence-Based Selection Criteria
Transparent Formulations Look for products listing individual ingredient amounts clearly. For berberine, this means seeing “Berberine HCl: 500mg” per capsule, not “Proprietary Metabolic Blend: 1000mg (contains berberine, cinnamon, chromium…).”
Research-supported dosages for key compounds: berberine (500mg, 2-3 times daily), glucomannan (2-4g before meals), psyllium (5-10g daily). If the product doesn’t provide enough of the active ingredient to match research doses, it’s unlikely to produce research-demonstrated effects.
Realistic, Evidence-Based Marketing Companies making modest claims supported by actual research citations—rather than pharmaceutical comparisons and transformation promises—demonstrate greater integrity. Marketing that acknowledges limitations and positions products as supportive tools rather than complete solutions aligns better with evidence.
Quality Certifications Third-party testing certifications verify ingredient identity, purity, and absence of contaminants. Look for marks from USP Verified, NSF International, Informed Choice, or similar independent testing programs. These certifications indicate the product contains what the label claims and lacks harmful contaminants 31Cohen, P.A. “The supplement paradox: negligible benefits, robust consumption.” JAMA, 2016; 316(14): 1453-1454..
For comprehensive guidance on evaluating supplement quality standards and understanding third-party testing certifications, see our supplement certifications comparison guide.
GMP (Good Manufacturing Practice) certification demonstrates basic manufacturing quality standards. Availability of Certificates of Analysis (COAs) showing batch-specific testing results indicates additional transparency.
Company Transparency Legitimate companies provide clear contact information, responsive customer service, and reasonable return policies. Educational content that acknowledges product limitations demonstrates more integrity than purely promotional marketing.
Compound-Specific Considerations
Berberine Products Effective berberine supplementation requires 500mg doses taken 2-3 times daily with meals—total daily intake of 1,000-1,500mg. Products providing lower doses or once-daily formulations may not deliver research-supported amounts. Berberine HCl and berberine sulfate are the best-studied forms.
Avoid mega-doses above 2,000mg daily, which increase side effect risk without additional benefit 32Yin, J. et al. “Efficacy of berberine in patients with type 2 diabetes mellitus.” Metabolism, 2008; 57(5): 712-717..
Fiber Products Effective fiber supplementation requires adequate dosing—5-10g per serving for metabolic effects. Products providing 1-2g per dose won’t produce satiety or microbiome benefits comparable to research studies.
Consider viscosity appropriate to your goal: glucomannan for satiety (highly viscous), inulin for prebiotic effects (fermentable), psyllium for combined benefits. Introduce gradually to minimize digestive discomfort.
Beyond supplement selection, building an effective metabolic health strategy requires understanding where these products fit—and where more fundamental interventions matter more.
Section 8: Building Your Metabolic Health Strategy
Understanding “GLP-1 booster” supplements matters most when placed in the broader context of effective metabolic health strategy. Supplements occupy a specific position in the evidence-based hierarchy—one that marketing often misrepresents.
The Evidence-Based Metabolic Health Hierarchy
Tier 1: Foundation (Non-Negotiable)
Metabolic health starts with fundamentals that produce effects orders of magnitude larger than any supplement:
Nutrition: Whole food emphasis, appropriate calorie balance for goals, adequate protein intake (1.6-2.2g/kg for active individuals), and high fiber consumption (25-38g daily) 33Volpe, S.L. “Magnesium and the Athlete.” Current Sports Medicine Reports, 2015; 14(4): 279-283.. These dietary factors influence insulin sensitivity, glucose metabolism, and satiety far more powerfully than metabolic supplements.
Physical Activity: Resistance training improves insulin sensitivity independent of weight loss 34Strasser, B. and Pesta, D. “Resistance training for diabetes prevention and therapy: experimental findings and molecular mechanisms.” BioMed Research International, 2013; 2013: 805217.. Cardiovascular exercise enhances metabolic flexibility. Daily movement counters sedentary metabolic dysfunction. Exercise produces metabolic benefits that supplements cannot replicate.
Sleep: Sleep deprivation acutely impairs glucose tolerance and insulin sensitivity 35Donga, E. et al. “A single night of partial sleep deprivation induces insulin resistance in multiple metabolic pathways in healthy subjects.” Journal of Clinical Endocrinology & Metabolism, 2010; 95(6): 2963-2968.. Chronic insufficient sleep (consistently <7 hours) significantly increases metabolic disease risk. Optimizing sleep likely provides greater metabolic benefit than any supplement intervention.
Stress Management: Chronic psychological stress elevates cortisol, impairs insulin signaling, and promotes visceral fat accumulation 36Hewagalamulage, S.D. et al. “Stress, cortisol, and obesity: a role for cortisol responsiveness in identifying individuals prone to obesity.” Domestic Animal Endocrinology, 2016; 56: S112-S120.. Addressing stress through practical strategies produces measurable metabolic improvements.
Tier 2: Lifestyle Optimization
Once foundation elements are consistent, lifestyle refinements provide incremental benefits: meal timing consistency, adequate hydration, minimizing environmental endocrine disruptors, and maintaining social connections that reduce chronic stress.
Tier 3: Targeted Supplementation (If Appropriate)
Only after establishing solid foundation and optimized lifestyle factors do supplements provide meaningful marginal gains:
- Address deficiencies first: Vitamin D, magnesium, or other documented nutritional gaps
- Evidence-based metabolic support: Berberine for metabolic syndrome, fiber for satiety, compounds with legitimate research for your specific context
- Individual response monitoring: Track measurable outcomes (fasting glucose, lipid panels, body composition), not subjective feelings or marketing promises
- Cost-benefit assessment: Are small improvements worth the financial investment and complexity?
Tier 4: Medical Intervention (When Indicated)
Clinical obesity, type 2 diabetes, or other metabolic conditions requiring pharmaceutical management represent appropriate medical intervention contexts. Supplements should complement, not replace, evidence-based medical treatment.
The Hierarchy Principle in Practice
Lower tiers must be solid before higher tiers matter. Berberine won’t compensate for poor sleep, inadequate protein intake, or sedentary behavior. Fiber supplements don’t fix a diet lacking whole foods. Marginal gains from supplementation only matter when fundamentals are in place.
Most people overestimate supplement impact while underestimating lifestyle factors. The metabolic benefit from consistent sleep exceeds the benefit from even the best-researched metabolic supplement. Marketing inverts this reality, suggesting supplements can deliver results that only comprehensive lifestyle change provides.
Practical Implementation
Start Here:
- Assess current nutrition, exercise, and sleep patterns honestly
- Identify the biggest gaps in your foundation
- Address lifestyle factors producing the largest metabolic impact
- Consider supplements only after foundation is consistently solid
If Pursuing Metabolic Support Supplements:
- Focus on evidence-based compounds: berberine (1,000-1,500mg daily), fiber (25-38g daily from food and supplements combined)
- Use research-supported doses, not under-dosed proprietary blends
- Give adequate trial periods (3 months minimum) with outcome tracking
- Monitor measurable markers: fasting glucose, HbA1c, lipid panels, body weight
- Discontinue if no measurable benefit after reasonable trial period
Personalized Supplement Strategy:
For evidence-based supplement recommendations tailored to your specific metabolic health goals, explore our Smart Stacks tool. Unlike generic “GLP-1 booster” products making pharmaceutical comparisons, Smart Stacks provides personalized recommendations based on your individual needs, properly dosed according to research, and positioned appropriately within your overall health strategy.
Long-Term Perspective
Metabolic health optimization is a marathon requiring sustainable approaches. Consistency with foundational behaviors matters more than perfect supplement selection. Habits you can maintain for years produce better outcomes than intensive interventions you abandon after weeks.
Reassess your strategy as new research emerges, your life circumstances change, and you gather data on your individual responses. What works evolves—remain flexible while maintaining evidence-based principles.
Understanding GLP-1 booster supplements in this broader context reveals why cutting through marketing noise matters—not just for avoiding ineffective products, but for focusing energy where it actually makes a difference.
Section 9: Conclusion
“GLP-1 booster” supplements represent a case study in how the supplement industry exploits pharmaceutical success for marketing advantage—and why cutting through that noise requires understanding both the science and the tactics.
What We’ve Established
The “GLP-1 booster” label is a marketing category, not a scientific classification. It groups together diverse compounds with different mechanisms under a single umbrella that implies pharmaceutical-like GLP-1 manipulation. Some of these compounds—particularly berberine and fiber—have legitimate metabolic effects supported by research. But these effects work through different mechanisms and produce dramatically smaller magnitudes than marketing comparisons to prescription GLP-1 agonists suggest.
Berberine’s primary metabolic benefits come through AMPK activation, not sustained GLP-1elevation. Fiber increases GLP-1 transiently while providing satiety and microbiome benefits. Other commonly included ingredients have weak or inconsistent evidence. None produce the continuous, pharmaceutical-level GLP-1 receptor activation that drives dramatic weight loss with medications like semaglutide.
The technical accuracy—”yes, this increases GLP-1″—creates misleading impressions when magnitude, duration, and biological significance remain unaddressed. A 20% increase in a hormone with a 2-minute half-life is fundamentally different from days-long pharmaceutical concentrations, regardless of pathway similarity.
Practical Application
If you’re considering supplements marketed as GLP-1 boosters, focus on individual compounds with actual evidence—particularly berberine (1,000-1,500mg daily) for metabolic syndrome support and fiber (25-38g daily) for satiety and gut health. Ignore the “GLP-1 booster” label and evaluate products based on ingredient transparency, appropriate dosing, third-party testing certifications, and realistic claims that acknowledge limitations.
Most importantly, remember that supplements provide marginal support within a foundation of solid nutrition, exercise, sleep, and stress management—not shortcuts around these fundamentals. The hierarchy matters: fix your sleep before optimizing your supplement stack. Establish consistent training before adding metabolic support compounds. Build dietary fiber intake from whole foods before considering supplements.
The Bigger Picture
The rapid emergence of “GLP-1 booster” supplements demonstrates how quickly the industry capitalizes on pharmaceutical breakthroughs—creating association without equivalence, borrowing credibility without delivering comparable results. This pattern isn’t unique to GLP-1 marketing; it’s a template the industry applies repeatedly as new scientific discoveries capture public attention.
Consumer protection in this environment requires critical thinking skills: understanding mechanism versus marketing, recognizing when technically accurate claims create false impressions, and evaluating products based on evidence rather than pharmaceutical associations. When you understand what these supplements actually do—modest metabolic support through primarily non-GLP-1 mechanisms—you can make informed decisions based on realistic expectations.
This is what cutting through the noise means: not dismissing supplements categorically, but understanding them accurately. Some people in specific contexts—metabolic syndrome, prediabetes, comprehensive health optimization—may benefit from evidence-based metabolic support supplements. But those benefits come from understanding the compounds themselves, not from believing marketing narratives that misrepresent their mechanisms and magnitudes.
For evidence-based supplement recommendations tailored to your specific health goals—properly dosed, transparently formulated, and positioned within comprehensive health strategy—explore our Smart Stacks tool. Because informed decisions require accurate information, not borrowed pharmaceutical credibility.
Frequently Asked Questions About GLP-1 Booster Supplements
Do GLP-1 booster supplements actually work?
Some compounds marketed as “GLP-1 boosters” have legitimate metabolic effects, but not through the mechanisms or magnitudes that marketing implies. Berberine consistently demonstrates modest improvements in glucose metabolism and insulin sensitivity through AMPK activation 37Lan, J. et al. “Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipemia and hypertension.” Journal of Ethnopharmacology, 2015; 161: 69-81.. Fiber supplements genuinely increase GLP-1 secretion transiently while providing satiety benefits.
What “work” means matters critically. If you’re seeking pharmaceutical-level weight loss (10-20% body weight reduction), these supplements won’t work. If you’re looking for modest metabolic support alongside comprehensive lifestyle changes—small improvements in fasting glucose, insulin sensitivity, and satiety—some evidence-based compounds may provide marginal benefits. The category label “GLP-1 booster” obscures more than it clarifies.
Is berberine really “nature’s Ozempic”?
No. This marketing claim fundamentally misrepresents both berberine’s mechanism and the magnitude of its effects.
Berberine primarily works through AMPK activation—the same pathway as metformin—improving insulin sensitivity and glucose metabolism 38Lee, Y.S. et al. “Berberine, a natural plant product, activates AMP-activated protein kinase with beneficial metabolic effects in diabetic and insulin-resistant states.” Diabetes, 2006; 55(8): 2256-2264.. While some studies show berberine can increase GLP-1 secretion modestly, this is a minor contributor to its metabolic effects, not the primary mechanism.
Semaglutide (Ozempic) produces average weight loss of 15% of body weight over 68 weeks 39Wilding, J.P. et al. “Once-weekly semaglutide in adults with overweight or obesity.” New England Journal of Medicine, 2021; 384(11): 989-1002.. Berberine meta-analyses show 2-3 pounds over 12 weeks—approximately 2-3% body weight in best-case scenarios 40Ye, Y. et al. “Efficacy and safety of berberine alone for several metabolic disorders: A systematic review and meta-analysis of randomized clinical trials.” Frontiers in Pharmacology, 2021; 12: 653887..
Berberine has legitimate metabolic benefits for people with insulin resistance or metabolic syndrome. Calling it “nature’s Ozempic” is marketing fiction. “Nature’s metformin” would be more accurate—and even that comparison overstates the similarity.
How much weight can I lose with GLP-1 booster supplements?
Realistic expectations based on research evidence:
Berberine: Meta-analyses show average weight loss of 1-3 pounds over 12 weeks in people with metabolic dysfunction 41Ye, Y. et al. “Efficacy and safety of berberine alone for several metabolic disorders: A systematic review and meta-analysis of randomized clinical trials.” Frontiers in Pharmacology, 2021; 12: 653887.. This represents 2-3% of body weight for a 150-pound individual—statistically significant but clinically modest.
Fiber supplements: Meta-analyses demonstrate approximately 2-3 pounds over several months 42Thompson, S.V. et al. “Effects of isolated soluble fiber supplementation on body weight, glycemia, and insulinemia in adults with overweight and obesity: a systematic review and meta-analysis of randomized controlled trials.” American Journal of Clinical Nutrition, 2017; 106(6): 1514-1528., primarily through satiety and calorie displacement rather than metabolic reprogramming.
For comparison:
- Consistent diet and exercise: 5-10% body weight over 6 months (evidence-based lifestyle programs)
- Pharmaceutical GLP-1 agonists: 10-20% body weight over 12-18 months
- Berberine/fiber supplements: 1-3 pounds over 3 months
Individual variation exists—some people respond better than others. But expecting double-digit weight loss from supplements marketed as “GLP-1 boosters” will lead to disappointment.
Are GLP-1 booster supplements safe?
Berberine is generally well-tolerated at standard doses (1,000-1,500mg daily), but carries important considerations:
- Common side effects: Gastrointestinal upset (cramping, diarrhea, constipation) in 10-30% of users, typically resolving within 2-4 weeks 43Yin, J. et al. “Efficacy of berberine in patients with type 2 diabetes mellitus.” Metabolism, 2008; 57(5): 712-717.
- Drug interactions: Can enhance blood glucose-lowering effects of diabetes medications (metformin, insulin), potentially causing hypoglycemia. May interact with medications metabolized by CYP3A4 enzymes
- Not recommended: During pregnancy, breastfeeding, or with certain liver conditions
Fiber supplements are safe for most people but require gradual introduction to minimize bloating and gas. Start with small doses and increase slowly over 2-3 weeks to allow gut adaptation.
General precautions: People taking prescription medications, those with diagnosed medical conditions, and individuals considering supplements as alternatives to medical treatment should coordinate with healthcare providers. These supplements are generally safe but not appropriate for everyone.
What’s the best GLP-1 booster supplement?
The question presumes “GLP-1booster” is a meaningful category—it’s not. Focus instead on individual compounds with actual evidence:
Most evidence-based options:
- Berberine (1,000-1,500mg daily): For metabolic syndrome support, insulin sensitivity improvement, modest glucose and lipid benefits
- Fiber supplements (25-38g daily total from food and supplements): For satiety, gut health, and transient GLP-1 increases
Product selection criteria:
- Transparent ingredient amounts (no proprietary blends)
- Research-supported dosing
- Third-party testing certifications (USP, NSF, Informed Choice)
- Realistic marketing without pharmaceutical comparisons
Rather than choosing based on “GLP-1 booster” labels, select evidence-based compounds appropriate to your specific metabolic needs. For personalized supplement recommendations based on your individual goals and health context, explore our Smart Stacks tool, which provides properly-dosed, evidence-based suggestions without misleading marketing claims.
Can I take GLP-1 supplements with prescription medications?
Berberine can interact with several medication classes:
- Diabetes medications: May enhance glucose-lowering effects, increasing hypoglycemia risk when combined with metformin, sulfonylureas, or insulin
- CYP3A4 substrates: Berberine inhibits this enzyme system, potentially affecting drugs metabolized through this pathway
- Anticoagulants: Possible interaction requiring monitoring
Fiber supplements can affect medication absorption if taken simultaneously. Take fiber supplements 1-2 hours before or after medications to minimize interference.
If you take prescription medications—particularly for diabetes, cardiovascular conditions, or other metabolic disorders—inform your healthcare provider before starting metabolic supplements. These products should complement medical treatment, not replace it. Never discontinue prescribed medications to try supplements marketed as “natural alternatives.”
How long does it take for GLP-1 supplements to work?
Timeline expectations based on research:
Berberine metabolic effects: 8-12 weeks for measurable improvements in fasting glucose, HbA1c, and lipid markers 44Lan, J. et al. “Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipemia and hypertension.” Journal of Ethnopharmacology, 2015; 161: 69-81.. Some individuals notice modest weight changes within 4-6 weeks, but clinically significant metabolic improvements require consistent use for at least 2-3 months.
Fiber supplements: Immediate satiety effects within days, but longer-term metabolic benefits (glucose metabolism, microbiome changes) develop over 8-12 weeks of consistent use.
Critical factors affecting timeline:
- Consistent dosing at research-supported amounts
- Baseline metabolic health (people with metabolic syndrome see more noticeable effects)
- Concurrent lifestyle factors (diet, exercise, sleep)
- Individual metabolic variation
Give any metabolic supplement a minimum 3-month trial with proper dosing before concluding whether it provides meaningful benefits. Track measurable outcomes (fasting glucose, body weight, energy levels) rather than relying on subjective impressions.
Do I need to diet and exercise if I take GLP-1 supplements?
Yes, absolutely. Supplements marketed as “GLP-1 boosters” cannot replace fundamental lifestyle factors.
The metabolic impact hierarchy clearly demonstrates that nutrition, exercise, sleep, and stress management produce effects orders of magnitude larger than any supplement intervention 45Strasser, B. and Pesta, D. “Resistance training for diabetes prevention and therapy: experimental findings and molecular mechanisms.” BioMed Research International, 2013; 2013: 805217.. Berberine’s modest metabolic benefits work best as support for comprehensive lifestyle changes, not as substitutes for absent foundational habits.
Consider the comparative effects:
- Poor sleep: Acutely impairs glucose tolerance and insulin sensitivity by 20-30%
- Sedentary behavior: Significantly reduces insulin sensitivity independent of weight
- Berberine supplementation: Improves glucose markers by 10-15% in best-case scenarios
You cannot supplement your way out of poor lifestyle habits. Build the foundation first—solid nutrition, consistent exercise, adequate sleep—then consider whether supplements provide marginal additional benefits worth pursuing.
Are there any side effects of GLP-1 booster supplements?
Berberine side effects:
- Gastrointestinal upset (most common): Cramping, diarrhea, constipation, or nausea in 10-30% of users, typically during first 2-4 weeks 46Yin, J. et al. “Efficacy of berberine in patients with type 2 diabetes mellitus.” Metabolism, 2008; 57(5): 712-717.
- Hypoglycemia risk: When combined with diabetes medications
- Drug interactions: With various medications metabolized through specific enzyme pathways
Fiber supplement side effects:
- Bloating and gas: Common when introduced too quickly or at excessive doses
- Digestive discomfort: Usually temporary, improves with gradual dose increases
- Medication interference: If taken simultaneously with prescriptions
General considerations: Most side effects are mild, temporary, and manageable with dose adjustment or gradual introduction. Starting with lower doses and increasing gradually minimizes gastrointestinal issues. Individual responses vary considerably—some people tolerate these supplements without any issues, while others experience persistent discomfort.
If side effects persist beyond 4 weeks or significantly affect quality of life, discontinue use. Supplements should support health, not create new problems.
Should I choose a multi-ingredient GLP-1 formula or single compounds?
Single compounds offer significant advantages:
Dosing clarity: You know exactly how much of each ingredient you’re taking, allowing verification against research-supported amounts
Cost-effectiveness: Multi-ingredient formulations often charge premium prices for under-dosed ingredients. Buying berberine and fiber separately typically costs less while providing effective doses
Targeted use: You can adjust individual compounds based on your specific needs and responses without changing entire formulations
Transparency: No proprietary blends hiding inadequate ingredient amounts
Problems with multi-ingredient “GLP-1 booster” formulas:
- Frequently use proprietary blends obscuring individual ingredient amounts
- Often contain multiple compounds at sub-effective doses
- Include ingredients with weak evidence to create impressive-sounding formulations
- Charge premium prices for formula sophistication rather than ingredient quality
Recommendation: Focus on evidence-based single compounds (berberine at 1,000-1,500mg daily, fiber at adequate doses) from reputable manufacturers with third-party testing rather than proprietary multi-ingredient formulas making pharmaceutical comparisons. Quality and appropriate dosing matter more than marketing sophistication.
References
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
- 22
- 23
- 24
- 25
- 26
- 27
- 28
- 29
- 30
- 31
- 32
- 33
- 34
- 35
- 36
- 37
- 38
- 39
- 40
- 41
- 42
- 43
- 44
- 45
- 46
This article is part of our Supplements hub — A science-backed collection of ingredient research, clinical dosage reviews, and optimized stack insights..
Questions or Comments?
If you have a question or comment about this article, feel free to leave it below. All comments are moderated for clarity, accuracy, and relevance.