Creatine Supplementation: The Complete Scientific Guide to Performance, Safety, and Optimal Usage
Abstract / Summary
This comprehensive guide represents the most current scientific understanding of creatine supplementation based on peer-reviewed research and clinical experience. All information is current as of 2025 and reflects the consensus of leading researchers and sports nutrition organizations worldwide.
Creatine stands as the most extensively researched and scientifically validated performance supplement in human history, with over 2,500 peer-reviewed studies demonstrating its efficacy across multiple domains of human performance, health, and disease states. With more research backing than any other dietary supplement, creatine monohydrate has earned recognition from major sports organizations, medical institutions, and regulatory bodies worldwide1Kreider, R.B., et al. “International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine.” Journal of the International Society of Sports Nutrition, 2017; 14: 18.https://doi.org/10.1186/s12970-017-0173-z. This unprecedented depth of scientific investigation has established creatine as the gold standard against which all other performance supplements are measured.
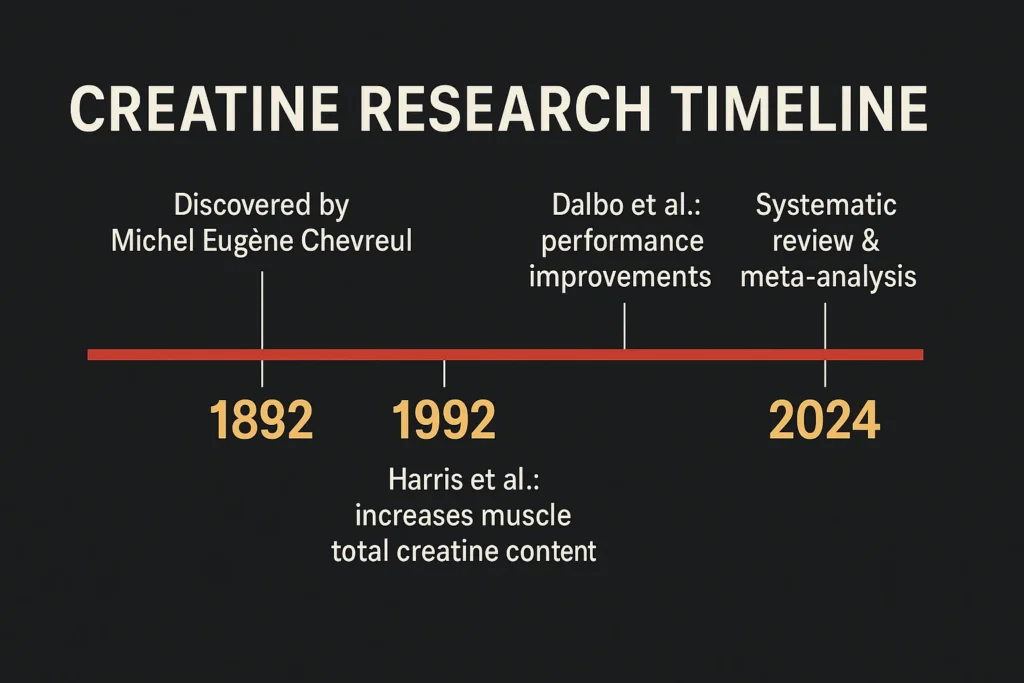
Unlike many supplements that rely on theoretical mechanisms or limited evidence, creatine’s benefits stem from fundamental cellular energy processes that have been mapped, measured, and validated through four decades of rigorous scientific investigation. From its initial discovery in 1832 by French scientist Michel Eugène Chevreul to the groundbreaking research of the 1990s that established its performance benefits, creatine represents one of the most thoroughly understood nutritional interventions in sports science.
This comprehensive analysis examines the current state of creatine research across all domains—from athletic performance and muscle physiology to cognitive enhancement and therapeutic applications. We explore optimal dosing protocols, individual variation factors, safety considerations across diverse populations, and emerging therapeutic applications that extend far beyond the gym and playing field.
The Evolutionary and Biochemical Foundation of Creatine
Evolutionary Perspective on Creatine Systems
The creatine-phosphocreatine system represents one of evolution’s most elegant solutions to the challenge of rapid energy delivery in metabolically demanding tissues. Present across virtually all vertebrate species, this system evolved as a critical adaptation enabling explosive movements essential for survival—escaping predators, capturing prey, and competing for mates2Wyss, M., & Kaddurah-Daouk, R. “Creatine and creatinine metabolism.” Physiological Reviews, 2000; 80(3): 1107-1213.https://doi.org/10.1152/physrev.2000.80.3.1107.
The evolutionary conservation of creatine kinase enzymes across species demonstrates their fundamental importance to cellular energy metabolism. From the electric organs of torpedo fish (containing the highest creatine concentrations in nature) to the flight muscles of hummingbirds, the creatine system enables rapid, high-power outputs that would be impossible through glycolysis or oxidative metabolism alone 3Wallimann, T., et al. “Intracellular compartmentation, structure and function of creatine kinase isoenzymes in tissues with high and fluctuating energy demands.” Biochemical Journal, 2011; 281(1): 21-40.https://doi.org/10.1042/bj2810021.
Human muscle contains approximately 120-140 mmol/kg dry weight of total creatine (creatine plus phosphocreatine), with elite power athletes sometimes reaching concentrations of 150-160 mmol/kg through training adaptations and genetic selection4Harris, R.C., et al. “Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation.” Clinical Science, 1992; 83(3): 367-374. https://doi.org/10.1042/cs0830367. This natural variation provides insight into the potential for optimization through supplementation and the individual differences observed in response patterns.
Detailed Biochemical Mechanisms
The Creatine Kinase Reaction
The fundamental reaction catalyzed by creatine kinase represents one of the most thermodynamically favorable processes in cellular metabolism:
PCr + ADP + H⁺ ↔ Cr + ATP
This reaction maintains ATP concentrations within the narrow physiological range (5-10 mM) required for cellular function during periods of high energy demand. The reaction’s reversibility allows phosphocreatine to serve dual roles as an energy buffer during high demand and an energy storage system during recovery periods5Bessman, S.P., & Geiger, P.J. “Transport of energy in muscle: the phosphorylcreatine shuttle.” Science, 1981; 211(4481): 448-452. https://doi.org/10.1126/science.6450446.
Multiple creatine kinase isoforms exist within muscle cells, each serving specific subcellular compartments:
- MM-CK (muscle-type): Cytosolic enzyme predominant in skeletal muscle
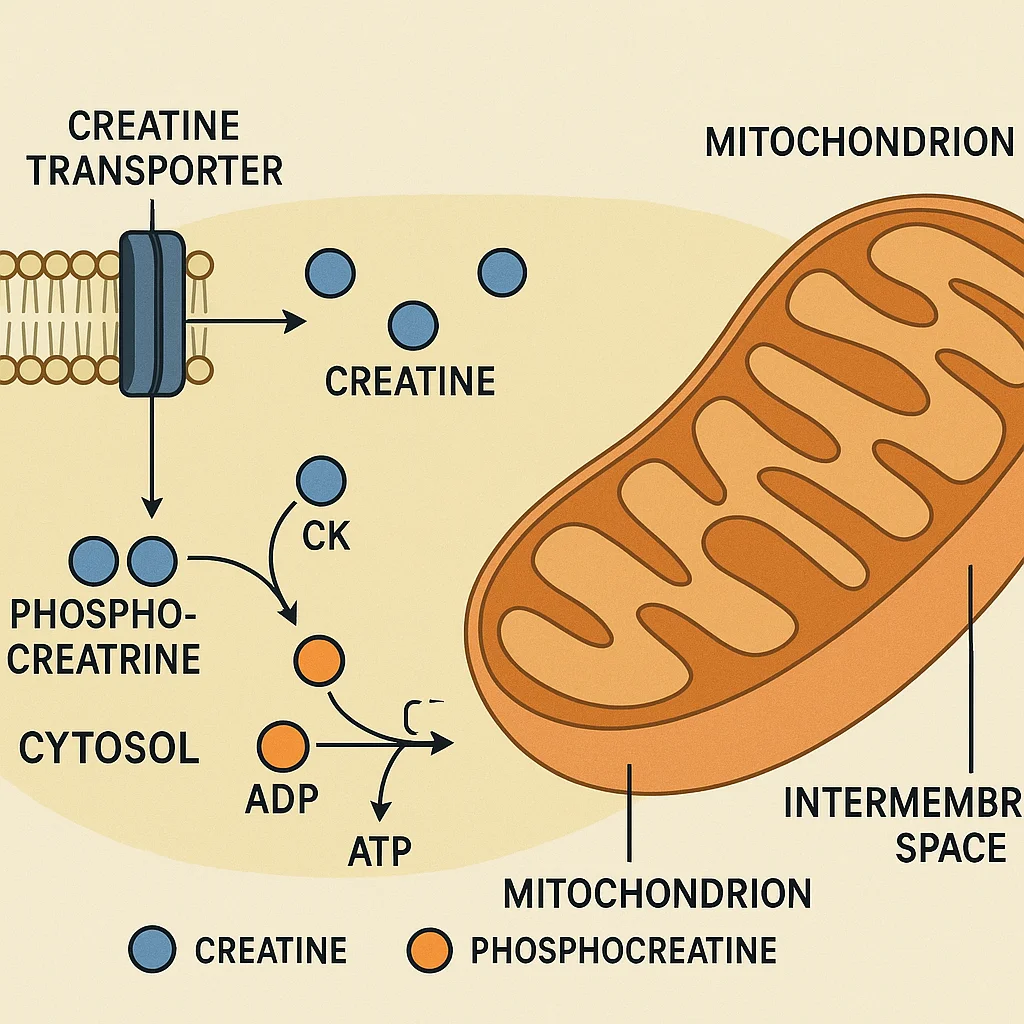
- Mt-CK (mitochondrial): Located in mitochondrial intermembrane space
- BB-CK (brain-type): Predominant in nervous tissue
- MB-CK: Hybrid form found in cardiac muscle
This compartmentalization creates localized energy networks that rapidly respond to ATP demands in specific cellular regions, particularly at myosin ATPase sites during muscle contraction6Schlattner, U., et al. “Mitochondrial creatine kinase in human health and disease.” Biochimica et Biophysica Acta, 2006; 1762(2): 164-180. https://doi.org/10.1016/j.bbadis.2005.09.004.
Cellular Transport and Regulation
Creatine entry into muscle cells occurs exclusively through the sodium- and chloride-dependent creatine transporter (CrT1, encoded by the SLC6A8 gene). This transporter exhibits Michaelis-Menten kinetics with a Km of approximately 20-50 μM, becoming saturated at plasma creatine concentrations achieved through supplementation7Guimbal, C., & Kilimann, M.W. “A Na(+)-dependent creatine transporter in rabbit brain, muscle, heart, and kidney.” Journal of Biological Chemistry, 1993; 268(12): 8418-8421. https://doi.org/10.1016/S0021-9258(18)52889-8.
The transport process is energy-dependent, requiring two sodium ions and one chloride ion per creatine molecule transported, creating a net positive charge influx that contributes to cellular depolarization. This coupling to sodium transport explains why creatine uptake increases with muscle activity and insulin stimulation, both of which activate sodium-potassium ATPase pumps8Snow, R.J., & Murphy, R.M. “Creatine and the creatine transporter: a review.” Molecular and Cellular Biochemistry, 2001; 224(1-2): 169-181. https://doi.org/10.1023/A:1011908606819.
Intracellular creatine regulation involves multiple feedback mechanisms:
- Creatine kinase activity: Regulated by ATP/ADP ratios and pH
- Creatine transporter expression: Downregulated by high intracellular creatine
- Endogenous synthesis: Inhibited by exogenous creatine supply
- Cellular efflux: Passive loss maintains steady-state levels
Tissue-Specific Creatine Systems
Skeletal Muscle Specializations
Type II (fast-twitch) muscle fibers contain significantly higher creatine concentrations than Type I (slow-twitch) fibers, reflecting their greater dependence on rapid energy turnover. This fiber-type specialization correlates with creatine kinase isoform expression, with fast fibers expressing higher levels of the MM-CK isoform optimized for rapid ATP regeneration9Greenhaff, P.L., et al. “Influence of oral creatine supplementation on muscle torque during repeated bouts of maximal voluntary exercise in man.” Clinical Science, 1993; 84(5): 565-571. https://doi.org/10.1042/cs0840565.
The spatial organization of creatine kinase within muscle cells creates “energy circuits” that directly couple ATP regeneration with utilization sites. MM-CK associates with myosin ATPase at the M-line of sarcomeres, while mitochondrial creatine kinase couples oxidative ATP production with phosphocreatine synthesis during recovery periods10Vendelin, M., et al. “Intracellular diffusion of adenosine phosphates is locally restricted in cardiac muscle.” Molecular and Cellular Biochemistry, 2004; 256-257(1-2): 229-241. https://doi.org/10.1023/B:MCBI.0000009871.04141.64.
Cardiac Muscle Adaptations
Cardiac muscle exhibits unique creatine metabolism characteristics that reflect its continuous, high-energy demands. Heart tissue maintains higher phosphocreatine/creatine ratios than skeletal muscle and expresses both mitochondrial and cytosolic creatine kinase isoforms in roughly equal proportions11Ingwall, J.S., et al. “The creatine kinase system in normal and diseased human myocardium.” New England Journal of Medicine, 1985; 313(17): 1050-1054. https://doi.org/10.1056/NEJM198510243131704.
The cardiac creatine system serves as both an energy buffer during systolic contraction and an energy transport mechanism moving high-energy phosphates from mitochondria to contractile proteins. Disruption of this system occurs in various cardiomyopathies and represents a target for therapeutic intervention12Neubauer, S. “The failing heart–an engine out of fuel.” New England Journal of Medicine, 2007; 356(11): 1140-1151. https://doi.org/10.1056/NEJMra063052.
Neural Tissue Specializations
Brain tissue contains the second-highest creatine concentrations in the body (approximately 5-10 mM), where it supports high-energy processes including neurotransmitter synthesis, ion transport, and synaptic transmission. The blood-brain barrier creatine transporter exhibits different kinetic properties than muscle transporters, with lower affinity but higher capacity13Braissant, O., et al. “Creatine deficiency syndromes and the importance of creatine synthesis in the brain.” Amino Acids, 2011; 40(5): 1315-1324. https://doi.org/10.1007/s00726-011-0852-z.
Regional variations in brain creatine content correlate with metabolic activity, with the highest concentrations in regions with dense synaptic activity such as the hippocampus, cerebellum, and frontal cortex. These patterns suggest specialized roles for creatine in cognitive processes and explain the cognitive benefits observed with supplementation14Béard, E., & Braissant, O. “Synthesis and transport of creatine in the CNS: importance for cerebral functions.” Journal of Neurochemistry, 2010; 115(2): 297-313. https://doi.org/10.1111/j.1471-4159.2010.06935.x.
Comprehensive Performance Benefits Across Training Domains
Strength and Power Development: Mechanisms and Applications
The relationship between creatine supplementation and strength/power development extends beyond simple energy system enhancement to include complex interactions with muscle protein synthesis, training volume capacity, and neuromuscular adaptations.
Primary Strength Adaptations
Creatine’s impact on maximal strength development occurs through multiple pathways:
- Acute force production: Enhanced ATP regeneration maintains peak force output during maximal efforts
- Training volume capacity: Improved recovery between sets allows greater total training stimulus
- Neuromuscular efficiency: Reduced fatigue maintains motor unit recruitment patterns
- Muscle protein synthesis: Enhanced training capacity drives superior adaptive responses
Meta-analyses spanning over 100 studies demonstrate consistent strength improvements of 5-15% across diverse populations and training protocols. The magnitude of improvement correlates with baseline strength levels, training status, and individual response patterns, with the greatest absolute gains observed in intermediate trainees15Branch, J.D. “Effect of creatine supplementation on body composition and performance: a meta-analysis.” International Journal of Sport Nutrition and Exercise Metabolism, 2003; 13(2): 198-226. https://doi.org/10.1123/ijsnem.13.2.198.
Power Output Enhancement
Peak power improvements with creatine supplementation typically exceed strength gains, reflecting the system’s specialization for rapid energy turnover. Studies examining various power assessments show:
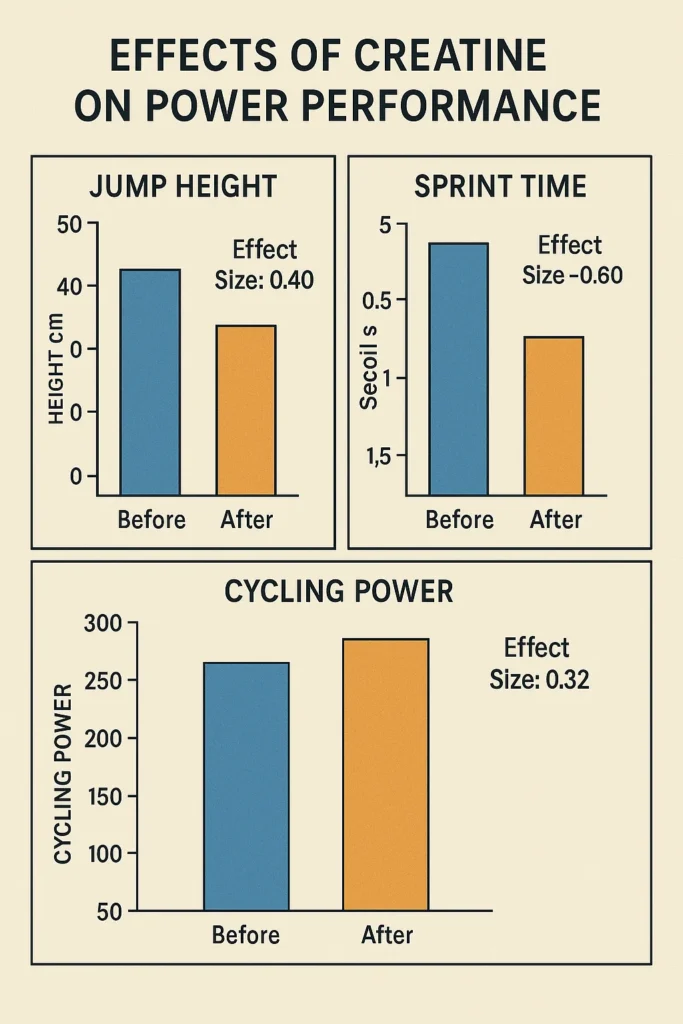
- Jump performance: 5-20% improvements in vertical jump height and power
- Sprint performance: 2-8% improvements in 10-100 meter sprint times
- Cycling power: 10-25% improvements in peak power output
- Throwing velocity: 3-12% improvements in various throwing sports
The time course of power improvements often occurs more rapidly than strength gains, with measurable benefits appearing within 5-7 days of loading protocols. This rapid response reflects the direct relationship between muscle phosphocreatine stores and peak power output capacity16Terjung, R.L., et al. “American College of Sports Medicine roundtable. The physiological and health effects of oral creatine supplementation.” Medicine & Science in Sports & Exercise, 2000; 32(3): 706-717. https://doi.org/10.1097/00005768-200003000-00024.
Resistance Training Volume Enhancement
Perhaps the most practically significant benefit of creatine supplementation involves enhanced training volume capacity. Studies consistently demonstrate that creatine users can perform more total repetitions, maintain higher loads across multiple sets, and recover more quickly between training sessions.
A landmark study by Volek et al. examined resistance-trained men performing bench press at 70% 1RM for multiple sets to failure. The creatine group completed significantly more total repetitions (15.4 ± 2.1 vs. 12.6 ± 1.8) and maintained performance better across successive sets17Volek, J.S., et al. “Performance and muscle fiber adaptations to creatine supplementation and heavy resistance training.” Medicine & Science in Sports & Exercise, 1999; 31(8): 1147-1156. https://doi.org/10.1097/00005768-199908000-00011. This enhanced training capacity translates to superior long-term adaptations in muscle mass, strength, and power.
The volume enhancement effect appears most pronounced during:
- Multiple set protocols: Benefits increase with set number
- Short rest intervals: 1-3 minute rest periods show greater effects
- Higher intensities: 70-90% 1RM loads demonstrate optimal benefits
- Complex movements: Multi-joint exercises show greater improvements
High-Intensity Interval Training and Repeated Sprint Performance
Creatine’s most dramatic performance benefits occur during activities characterized by repeated high-intensity efforts with brief recovery periods—precisely the scenario encountered in most team sports and high-intensity interval training protocols.
Physiological Mechanisms in HIIT
During repeated sprint efforts, muscle phosphocreatine stores deplete rapidly (50-70% within 10 seconds of maximal effort) and recover slowly during brief rest intervals (50% recovery in 30 seconds, 85% in 2 minutes). Creatine supplementation enhances both the initial phosphocreatine stores and the rate of resynthesis during recovery periods18Balsom, P.D., et al. “Skeletal muscle metabolism during short duration high-intensity exercise: influence of creatine supplementation.” Acta Physiologica Scandinavica, 1995; 154(3): 303-310. https://doi.org/10.1111/j.1748-1716.1995.tb09914.x.
The enhanced phosphocreatine resynthesis occurs through improved coupling between mitochondrial ATP production and cytosolic phosphocreatine regeneration via the creatine kinase shuttle system. This mechanism explains why creatine benefits extend beyond the duration of the phosphocreatine system alone19Casey, A., et al. “Creatine ingestion favorably affects performance and muscle metabolism during maximal exercise in humans.” American Journal of Physiology, 1996; 271(1): E31-E37. https://doi.org/10.1152/ajpendo.1996.271.1.E31.
Team Sport Applications
Team sports present unique physiological demands that align perfectly with creatine’s performance profile. Activities like soccer, basketball, hockey, and rugby involve repeated high-intensity efforts (sprints, jumps, direction changes) interspersed with lower-intensity recovery periods.
Research in elite female soccer players demonstrated that creatine supplementation improved performance during a field test simulating match conditions, with benefits most apparent in the later stages when fatigue typically accumulates20Cox, G., et al. “Acute creatine supplementation and performance during a field test simulating match play in elite female soccer players.” International Journal of Sport Nutrition and Exercise Metabolism, 2002; 12(1): 33-46. https://doi.org/10.1123/ijsnem.12.1.33. Similar improvements have been documented across various team sports:
- Soccer: Improved sprint times, jump height, and skill execution
- Basketball: Enhanced vertical jump maintenance and sprint performance
- Hockey: Better acceleration and top speed maintenance
- Rugby: Improved power output in scrums and rucks
Swimming and Aquatic Sports
Swimming represents an ideal testing ground for creatine benefits due to the sport’s emphasis on repeated high-intensity efforts and the ability to precisely measure performance changes. Studies in competitive swimmers consistently demonstrate improved performance in sprint events and training sets.
Peyrebrune et al. examined elite swimmers performing six 50-meter freestyle sprints with 4-minute recovery intervals. The creatine group maintained sprint times across all six efforts, while the placebo group showed progressive performance deterioration21Peyrebrune, M.C., et al. “The effects of oral creatine supplementation on performance in single and repeated sprint swimming.” Journal of Sports Sciences, 1998; 16(3): 271-279. https://doi.org/10.1080/026404198366794. This maintenance of speed during repeated efforts translates directly to improved training quality and competitive performance.
Cycling Power and Endurance
While cycling presents mixed demands across different event durations, creatine supplementation provides clear benefits for events lasting 30 seconds to 6 minutes, where both phosphocreatine and glycolytic systems contribute significantly to energy production.
Time trial performance improvements with creatine supplementation show a clear relationship with event duration:
- 30-60 seconds: 5-12% improvement
- 1-4 minutes: 2-8% improvement
- 4-10 minutes: 1-4% improvement
- >10 minutes: Minimal direct benefit
These findings reflect the progressive shift from phosphocreatine dependence to oxidative metabolism as exercise duration increases22Chwalbinska-Moneta, J. “Effect of creatine supplementation on aerobic performance and anaerobic capacity in elite rowers in the course of endurance training.” International Journal of Sport Nutrition and Exercise Metabolism, 2003; 13(2): 173-183. https://doi.org/10.1123/ijsnem.13.2.173.
Strength Training Adaptations and Muscle Hypertrophy
Beyond acute performance benefits, creatine supplementation enhances long-term training adaptations through multiple mechanisms that extend the supplement’s effects beyond its direct energy system impacts.
Enhanced Training Stimulus
The primary driver of muscle hypertrophy involves progressive overload—the systematic increase in training demands over time. Creatine supplementation enhances the ability to apply progressive overload through:
- Increased training volume: More total repetitions and sets per session
- Maintained intensity: Less performance decline across training sessions
- Improved recovery: Faster restoration of performance between sessions
- Enhanced motivation: Reduced perceived exertion during training
Studies examining long-term resistance training with creatine supplementation consistently demonstrate superior gains in muscle mass compared to training alone. A 6-week study in resistance-trained men showed that creatine supplementation enhanced lean body mass gains by approximately 60% compared to placebo (2.2 kg vs. 1.4 kg)23Willoughby, D. S., & Rosene, J. (2001). Effects of oral creatine and resistance training on myosin heavy chain expression. Medicine & Science in Sports & Exercise, 33(10), 1674-1681.https://doi.org/10.1097/00005768-200110000-00010.
Muscle Protein Synthesis Enhancement
Recent research suggests that creatine may directly influence muscle protein synthesis pathways beyond its effects on training capacity. Proposed mechanisms include:
- mTOR activation: Creatine may enhance mTOR signaling in response to resistance exercise
- Cellular hydration: Increased cell volume may trigger anabolic signaling cascades
- IGF-1 upregulation: Some studies suggest enhanced growth factor expression
- Reduced protein breakdown: Potential anti-catabolic effects during intense training
While these mechanisms require further investigation, the consistent observation of enhanced muscle growth with creatine supplementation suggests effects beyond simple training volume improvements24Deldicque, L., et al. “Increased IGF mRNA in human skeletal muscle after creatine supplementation.” Medicine & Science in Sports & Exercise, 2005; 37(5): 731-736. https://doi.org/10.1249/01.MSS.0000162690.39830.27.
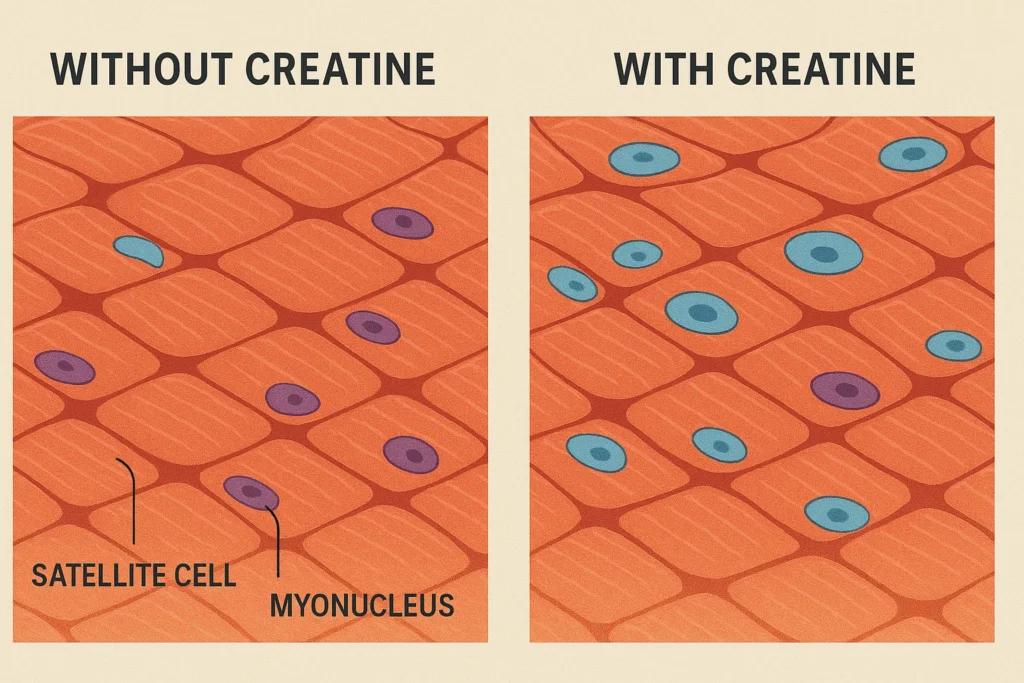
Satellite Cell Activation
Muscle growth ultimately depends on satellite cell activation and fusion with existing muscle fibers. Creatine supplementation may enhance this process through improved cellular energy status and reduced exercise-induced muscle damage.
Studies using muscle biopsy techniques demonstrate that creatine supplementation increases satellite cell number and myonuclei number per muscle fiber following resistance training. These cellular adaptations provide the foundation for sustained muscle growth and strength development25Olsen, S., et al. “Creatine supplementation augments the increase in satellite cell and myonuclei number in human skeletal muscle induced by strength training.” Journal of Physiology, 2006; 573(2): 525-534. https://doi.org/10.1113/jphysiol.2006.107359.
Advanced Dosing Protocols and Optimization Strategies
Classical Loading vs. Modern Approaches
The evolution of creatine dosing protocols reflects advancing understanding of muscle creatine kinetics, individual variation, and practical considerations for different user populations.
Traditional Loading Protocol Development
The classical 20-25 gram loading protocol emerged from early research by Harris et al., who first demonstrated the feasibility of increasing muscle creatine stores through oral supplementation26Hultman, E., et al. “Muscle creatine loading in men.” Journal of Applied Physiology, 1996; 81(1): 232-237. https://doi.org/10.1152/jappl.1996.81.1.232. This approach was designed to rapidly saturate muscle creatine transporters and achieve maximal muscle creatine content within 5-7 days.
The physiological rationale for loading involves overcoming the limited capacity of creatine transporters through sustained high plasma concentrations. During loading, plasma creatine levels reach 200-300 times normal concentrations, driving maximal transporter activity despite saturation kinetics27Harris, R.C., et al. “The time course of phosphocreatine resynthesis during recovery of the quadriceps muscle in man.” Pflügers Archiv, 1976; 367(2): 137-142. https://doi.org/10.1007/BF00585149.
Loading protocol specifics:
- Dose: 0.3 g/kg body weight daily (typically 20-25g)
- Frequency: 4-5 divided doses throughout the day
- Duration: 5-7 days
- Timing: With meals to minimize gastrointestinal distress
- Transition: Followed by 3-5g daily maintenance
Non-Loading Alternatives
Recognition that loading protocols can cause gastrointestinal distress and may be unnecessary for achieving long-term benefits led to development of alternative approaches. Research demonstrates that 3-5 grams daily achieves identical muscle creatine saturation over 3-4 weeks without the potential side effects of high-dose protocols28Burke, D.G., et al. “Effect of creatine and weight training on muscle creatine and performance in vegetarians.” Medicine & Science in Sports & Exercise, 2003; 35(11): 1946-1955. https://doi.org/10.1249/01.MSS.0000093614.17517.79.
Non-loading advantages:
- Reduced GI distress: Lower incidence of stomach upset and diarrhea
- Improved compliance: Easier to maintain consistent supplementation
- Cost effectiveness: Lower daily supplement costs during initial phase
- Practical simplicity: Single daily dose vs. multiple divided doses
The choice between loading and non-loading approaches should be individualized based on:
- Timeline needs: Loading for rapid benefits, non-loading for gradual improvement
- GI sensitivity: Non-loading for sensitive individuals
- Training schedule: Loading before competition peaks or training camps
- Experience level: Non-loading for first-time users
Body Weight and Composition Considerations
Lean Body Mass-Based Dosing
Traditional dosing recommendations based on total body weight fail to account for the fact that creatine primarily accumulates in metabolically active tissues, particularly skeletal muscle. Research suggests that lean body mass provides a more accurate basis for dosing calculations29Syrotuik, D.G., & Bell, G.J. “Acute creatine monohydrate supplementation: a descriptive physiological profile of responders vs. non-responders.” Journal of Strength and Conditioning Research, 2004; 18(3): 610-617.
For practical application: Muscle Fiber Type Considerations Individual variation in muscle fiber type distribution significantly influences creatine response patterns and may warrant dosing adjustments. Type II (fast-twitch) fibers contain higher creatine concentrations and demonstrate greater response to supplementation compared to Type I (slow-twitch) fibers30Kilduff, L.P., et al. “The effects of creatine supplementation on cardiovascular, metabolic, and thermoregulatory responses during exercise in the heat in endurance-trained humans.” International Journal of Sport Nutrition and Exercise Metabolism, 2004; 14(4): 443-460. https://doi.org/10.1123/ijsnem.14.4.443. Athletes with predominantly fast-twitch fiber types (sprinters, powerlifters, bodybuilders) may benefit from higher maintenance doses (5-7g daily), while endurance athletes with greater slow-twitch fiber predominance may require lower doses (3-4g daily) for optimal cost-effectiveness. Post-Exercise Optimization While muscle creatine uptake occurs independently of exercise timing over long-term supplementation periods, acute research suggests modest benefits from post-exercise consumption, particularly when combined with carbohydrates or protein31Antonio, J., & Ciccone, V. “The effects of pre versus post workout supplementation of creatine monohydrate on body composition and strength.” Journal of the International Society of Sports Nutrition, 2013; 10(1): 36. https://doi.org/10.1186/1550-2783-10-36. Proposed mechanisms for post-exercise benefits: Practical post-exercise protocol: Carbohydrate Co-ingestion Protocols Carbohydrate co-ingestion enhances muscle creatine uptake through insulin-mediated improvements in transporter activity. The effective dose appears to be approximately 80-100g of carbohydrates per 5g of creatine, though lower doses (20-40g) provide meaningful benefits with reduced caloric impact32Green, A.L., et al. “Carbohydrate ingestion augments skeletal muscle creatine accumulation during creatine supplementation in humans.” American Journal of Physiology, 1996; 271(5): E821-E826. https://doi.org/10.1152/ajpendo.1996.271.5.E821. Optimal carbohydrate characteristics: Protein Co-ingestion Benefits Protein co-ingestion with creatine may provide synergistic benefits for muscle protein synthesis and training adaptations beyond simple creatine uptake enhancement. The combination appears particularly beneficial when consumed post-exercise33Stout, J., et al. “Effects of creatine supplementation on the onset of neuromuscular fatigue threshold and muscle strength in elderly men and women (64-86 years).” Journal of Nutrition, Health & Aging, 1999; 3(4): 226-233. PMID: 10885806. Proposed synergistic mechanisms: Practical protein co-ingestion: Athletic Population Protocols Different athletic populations may benefit from tailored creatine protocols based on training demands, competition schedules, and performance goals. Power/Strength Athletes: Team Sport Athletes: Endurance Athletes: Aging Population Considerations Older adults demonstrate altered creatine kinetics that may warrant modified supplementation approaches. Age-related changes include reduced muscle mass, decreased creatine transporter expression, and altered training capacity34Candow, D.G., et al. “Effect of creatine supplementation during resistance training on lean tissue mass and muscular strength in older adults: a meta-analysis.” Open Access Journal of Sports Medicine, 2014; 5: 25-34. https://doi.org/10.2147/OAJSM.S40893. Modified protocols for older adults: Vegetarian Population Optimization Vegetarians and vegans demonstrate significantly lower baseline muscle creatine levels due to absent dietary creatine intake from meat sources. This population consistently shows the greatest response to creatine supplementation and may require modified protocols35Shomrat, A., et al. “Effect of creatine feeding on maximal exercise performance in vegetarians.” European Journal of Applied Physiology, 2000; 82(4): 321-325. https://doi.org/10.1007/s004210000222. Vegetarian-specific considerations: The safety profile of creatine monohydrate has been established through extensive clinical investigation spanning acute high-dose studies, medium-term athletic population research, and long-term health monitoring across diverse demographics. Gastrointestinal Effects and Management Gastrointestinal distress represents the most commonly reported adverse effect of creatine supplementation, occurring in approximately 5-15% of users during loading phases and 1-3% during maintenance dosing. The manifestations include nausea, stomach cramping, diarrhea, and general abdominal discomfort36Poortmans, J.R., & Francaux, M. “Adverse effects of creatine supplementation: fact or fiction?” Sports Medicine, 2000; 30(3): 155-170. https://doi.org/10.2165/00007256-200030030-00002. The mechanisms underlying GI distress involve: Evidence-based management strategies: Weight Gain Patterns and Body Composition Changes Weight gain consistently occurs with creatine supplementation, typically ranging from 0.5-2.0 kg within the first 1-2 weeks. This weight increase reflects enhanced intracellular water retention rather than fat accumulation and generally stabilizes after the initial adaptation period37Powers, M.E., et al. “Creatine supplementation increases total body water without altering fluid distribution.” Journal of Athletic Training, 2003; 38(1): 44-50. PMC155510. Detailed body composition analysis reveals: The time course of weight gain follows predictable patterns: For athletes in weight-class sports, this weight gain requires consideration during competition preparation. However, the enhanced training capacity typically outweighs temporary weight increases for most athletic applications38Ziegenfuss, T.N., et al. “Effect of creatine loading on anaerobic performance and skeletal muscle volume in NCAA Division I athletes.” Nutrition, 2002; 18(5): 397-402. https://doi.org/10.1016/S0899-9007(01)00802-4. Dehydration and Thermoregulation Concerns Early theoretical concerns suggested that creatine-induced cellular water retention might impair thermoregulation and increase dehydration risk during exercise in hot conditions. Extensive research has thoroughly investigated these concerns across various environmental conditions and exercise protocols. Comprehensive meta-analysis of heat tolerance studies demonstrates no increased risk of heat illness, dehydration, or impaired thermoregulation with creatine supplementation when adequate fluid intake is maintained39Lopez, R.M., et al. “Does creatine supplementation hinder exercise heat tolerance or hydration status? A systematic review with meta-analyses.” Journal of Athletic Training, 2009; 44(2): 215-223. https://doi.org/10.4085/1062-6050-44.2.215. Key findings include: Practical hydration guidelines for creatine users: Renal Function: Comprehensive Analysis Kidney safety represents the most thoroughly investigated aspect of long-term creatine supplementation, driven by early case reports suggesting potential nephrotoxicity and the theoretical concern that increased creatine turnover might stress renal function40Thorsteinsdottir, B., et al. “The renal safety of upper-level creatine monohydrate supplementation.” Clinical Journal of Sport Medicine, 2006; 16(2): 142-148. https://doi.org/10.1097/00042752-200603000-00009. Mechanistic Understanding: Creatine metabolism produces creatinine as a waste product at a rate of approximately 1-2% of total body creatine per day. Supplementation increases creatine stores by 10-40%, theoretically increasing creatinine production proportionally. However, this increase occurs within the normal physiological range and does not represent pathological kidney stress41Persky, A.M., et al. “Clinical pharmacology of the dietary supplement creatine monohydrate.” Pharmacological Reviews, 2001; 53(2): 161-176. https://doi.org/10.1124/pr.53.2.161. Clinical Evidence Base: Multiple systematic reviews and meta-analyses have examined kidney function markers in creatine users across various populations and durations: The largest long-term safety study followed 175 athletes using creatine for up to 5 years, measuring comprehensive kidney function markers every 3 months. No participant showed evidence of kidney dysfunction, and group mean values remained within normal ranges throughout the study period42Kreider, R.B., et al. “Long-term creatine supplementation does not significantly affect clinical markers of health in athletes.” Molecular and Cellular Biochemistry, 2003; 244(1-2): 95-104. https://doi.org/10.1023/A:1022469320296. Special Population Considerations: Creatinine Elevation Interpretation: Modest increases in serum creatinine (typically 10-20% above baseline) occasionally occur with creatine supplementation but reflect increased creatine turnover rather than kidney dysfunction. Key distinguishing features: Hepatic Function and Metabolism Liver safety has received less attention than kidney function but remains important given the liver’s role in creatine synthesis and metabolism. Available evidence suggests no adverse effects on liver function with standard creatine supplementation protocols43Gualano, B., et al. “Creatine supplementation and renal function: systematic review and meta-analysis.” European Journal of Sport Science, 2015; 15(1): 26-39. https://doi.org/10.1080/17461391.2014.966806. Creatine’s hepatic effects include: Studies in populations with elevated baseline liver stress (intense training, alcohol consumption) show no additional hepatic burden from creatine supplementation. Liver function markers including ALT, AST, bilirubin, and albumin remain within normal ranges during both short and long-term supplementation44Kreider, R.B. “Effects of creatine supplementation on performance and training adaptations.” Molecular and Cellular Biochemistry, 2003; 244(1-2): 89-94. https://doi.org/10.1023/A:1022465203458. Cardiovascular Safety Profile Cardiovascular safety represents an important consideration given creatine’s effects on fluid balance, exercise capacity, and potential interactions with cardiac medications. Comprehensive investigation reveals an excellent cardiovascular safety profile with potential protective effects45Schroder, H., et al. “A short-term creatine supplementation does not alter plasma homocysteine levels in humans.” Journal of Nutrition, 2005; 135(12): 2882-2886. https://doi.org/10.1093/jn/135.12.2882. Blood Pressure Effects: Multiple studies examining blood pressure responses to creatine supplementation show: Cardiac Function: Echocardiographic studies in athletes using creatine supplementation demonstrate: Lipid Profile Effects: Research examining blood lipid changes with creatine supplementation shows neutral to beneficial effects: Pharmaceutical Interactions Creatine demonstrates minimal potential for clinically significant drug interactions due to its unique transport and metabolic pathways. However, several theoretical interactions warrant consideration in clinical practice46Buford, T.W., et al. “International Society of Sports Nutrition position stand: creatine supplementation and exercise.” Journal of the International Society of Sports Nutrition, 2007; 4: 6. https://doi.org/10.1186/1550-2783-4-6. Nephrotoxic Medications: While direct interactions have not been documented, theoretical concerns exist regarding concurrent use of creatine with medications that can affect kidney function: Diabetes Medications: Some research suggests creatine may influence glucose metabolism, requiring monitoring in diabetic individuals using glucose-lowering medications: Stimulant Interactions: The relationship between creatine and caffeine remains controversial, with conflicting research results: Contraindications and Precautions Absolute Contraindications (limited evidence but prudent avoidance): Relative Contraindications (requiring medical supervision): Enhanced Monitoring Recommendations: The substantial individual variation observed in creatine supplementation studies (ranging from non-responders showing minimal benefit to high-responders achieving 40+ % performance improvements) stems from complex genetic, physiological, and behavioral factors that are increasingly well-understood through molecular research47Deldicque, L., et al. “Creatine supplementation and the transcriptomic response to resistance exercise.” American Journal of Physiology-Endocrinology and Metabolism, 2008; 294(1): E184-E189. https://doi.org/10.1152/ajpendo.00466.2007. Creatine Transporter Genetics The SLC6A8 gene encoding the creatine transporter exhibits multiple polymorphisms that significantly influence transport capacity and supplementation response. Research has identified several key variants that affect both baseline muscle creatine levels and response to supplementation48Peral, M.J., et al. “Human, rat and chicken small intestinal Na+-Cl–creatine transporter: functional, molecular characterization and localization.” Journal of Physiology, 2002; 545(1): 133-144. https://doi.org/10.1113/jphysiol.2002.026377. Common SLC6A8 Polymorphisms: Individuals carrying certain polymorphic variants demonstrate: Creatine Kinase Isoform Genetics Multiple genes encode different creatine kinase isoforms, with polymorphisms affecting enzyme activity, subcellular localization, and thermal stability. The most significant variants include: CKM Gene (Muscle Creatine Kinase): CKMT1A/CKMT1B Genes (Mitochondrial Creatine Kinase): These genetic variations help explain why some individuals show dramatic performance improvements while others experience minimal benefits despite similar supplementation protocols and baseline fitness levels49Salomons, G.S., et al. “X-linked creatine-transporter gene (SLC6A8) defect: a new creatine-deficiency syndrome.” American Journal of Human Genetics, 2001; 68(6): 1497-1500. https://doi.org/10.1086/320595. Muscle Fiber Type Genetic Determinants The proportion of Type I (slow-twitch) versus Type II (fast-twitch) muscle fibers significantly influences creatine response patterns. Genetic variants affecting fiber type distribution include: ACTN3 Gene (Alpha-Actinin-3): MLCK Gene (Myosin Light Chain Kinase): MCT1 Gene (Monocarboxylate Transporter): Baseline Muscle Creatine Levels Perhaps the strongest predictor of creatine supplementation response involves baseline muscle creatine content, which varies substantially between individuals due to genetic, dietary, and training factors50Greenhaff, P.L., et al. “Effect of oral creatine supplementation on skeletal muscle phosphocreatine resynthesis.” American Journal of Physiology, 1994; 266(5): E725-E730. https://doi.org/10.1152/ajpendo.1994.266.5.E725. Measurement and Assessment: Direct measurement of muscle creatine requires invasive muscle biopsy procedures, making clinical assessment impractical. However, indirect indicators can provide insights: Response Prediction: Individuals with lower baseline creatine levels consistently demonstrate the greatest absolute and relative improvements with supplementation: Training Status and Athletic Background Training history and current fitness level significantly influence both baseline creatine levels and response to supplementation, creating complex interactions that affect optimal protocols51Rawson, E.S., & Volek, J.S. “Effects of creatine supplementation and resistance training on muscle strength and weightlifting performance.” Journal of Strength and Conditioning Research, 2003; 17(4): 822-831.
Recreational Athletes: Elite Athletes: Detraining Effects: Athletes transitioning from high training volumes to reduced activity show altered creatine kinetics: Vegetarian and Vegan Populations Vegetarians and vegans represent a unique population for creatine research due to their complete absence of dietary creatine intake from meat sources. This creates a natural experiment in creatine deficiency and supplementation response52Watt, K.K., et al. “Effect of creatine supplementation on body composition and performance measures in a vegetarian population.” International Journal of Sport Nutrition and Exercise Metabolism, 2004; 14(6): 643-656. https://doi.org/10.1123/ijsnem.14.6.643. Baseline Differences: Comprehensive studies comparing vegetarians to omnivores reveal: Supplementation Response: Vegetarians consistently demonstrate the most dramatic responses to creatine supplementation: Practical Implications: Carbohydrate Intake Patterns Dietary carbohydrate intake influences creatine uptake through insulin-mediated effects on muscle creatine transporters. Individuals with different carbohydrate consumption patterns show variable responses to supplementation53Steenge, G.R., et al. “Stimulatory effect of insulin on creatine accumulation in human skeletal muscle.” American Journal of Physiology, 1998; 275(6): E974-E979. https://doi.org/10.1152/ajpendo.1998.275.6.E974. High-Carbohydrate Diets (>5g/kg body weight daily): Low-Carbohydrate Diets (<2g/kg body weight daily): Ketogenic Diets: Hydration Status and Fluid Intake Chronic hydration status influences creatine supplementation effectiveness through multiple mechanisms involving cellular transport, kidney function, and performance outcomes54Watson, G., et al. “Creatine use and exercise heat tolerance in dehydrated men.” Journal of Athletic Training, 2006; 41(1): 18-29. PMC1421488. Optimal Hydration Effects: Dehydration Interactions: Objective Performance Measures Systematic monitoring of creatine supplementation effectiveness requires objective, reproducible measures that reflect the supplement’s primary mechanisms of action55Hoffman, J.R., et al. “Effect of creatine and beta-alanine supplementation on performance and endocrine responses in strength/power athletes.” International Journal of Sport Nutrition and Exercise Metabolism, 2006; 16(4): 430-446. https://doi.org/10.1123/ijsnem.16.4.430. Strength and Power Assessments: Training Volume Metrics: Recovery Indicators: Biochemical and Physiological Markers While not practical for most users, certain biomarkers can provide insights into creatine supplementation effectiveness and individual response patterns56Vandenberghe, K., et al. “Long-term creatine intake is beneficial to muscle performance during resistance training.” Journal of Applied Physiology, 1997; 83(6): 2055-2063. https://doi.org/10.1152/jappl.1997.83.6.2055. Accessible Markers: Clinical Markers (for research or medical supervision): Timeline for Response Assessment Understanding the expected timeline for creatine benefits helps set realistic expectations and determine individual response status57Rawson, E.S., & Venezia, A.C. “Use of creatine in the elderly and evidence for effects on cognitive function in young and old.” Amino Acids, 2011; 40(5): 1349-1362. https://doi.org/10.1007/s00726-011-0855-9. Acute Phase (Days 1-7): Adaptation Phase (Weeks 1-4): Maintenance Phase (Month 2+): Creatine monohydrate represents not merely the original form of creatine supplement, but the compound used in over 95% of published research demonstrating safety and efficacy benefits. Its status as the reference standard stems from decades of investigation, pharmaceutical-grade manufacturing processes, and consistent clinical outcomes across diverse populations and applications58Jäger, R., et al. “Analysis of the efficacy, safety, and regulatory status of novel forms of creatine.” Amino Acids, 2011; 40(5): 1369-1383. https://doi.org/10.1007/s00726-010-0729-5. Chemical and Physical Properties: Creatine monohydrate (C₄H₉N₃O₂·H₂O) consists of creatine bound to a single water molecule, creating a stable crystalline structure that maintains potency under normal storage conditions. The monohydrate form contains approximately 88% creatine by weight, with the remaining 12% comprising the water molecule integral to its structure59Gufford, B.T., et al. “Physicochemical characterization of creatine N-methylguanidinium salts.” Journal of Dietary Supplements, 2010; 7(3): 240-252. https://doi.org/10.3109/19390211.2010.508034. Key characteristics include: Manufacturing and Quality Standards: High-quality creatine monohydrate production involves multi-step chemical synthesis followed by purification and crystallization processes. The leading manufacturers employ pharmaceutical-grade production standards that ensure consistent purity and potency60Ganguly, S., et al. “Analysis of the chemical stability of creatine in solution prepared from effervescent creatine formulations.” AAPS PharmSciTech, 2003; 4(2): E25. https://doi.org/10.1208/pt040225. Quality indicators include: Research Foundation: The extensive research base supporting creatine monohydrate includes: This research foundation provides unparalleled confidence in creatine monohydrate’s risk-benefit profile compared to alternative forms with limited investigation61Gualano, B., et al. “Exploring the therapeutic role of creatine supplementation.” Amino Acids, 2012; 43(1): 25-35. https://doi.org/10.1007/s00726-011-1132-7. The supplement industry has developed numerous alternative creatine formulations claiming enhanced absorption, reduced side effects, improved solubility, or superior performance benefits. However, the scientific evidence supporting these claims remains limited, inconsistent, or contradictory to marketing assertions62Spillane, M., et al. “The effects of creatine ethyl ester supplementation combined with heavy resistance training on body composition, muscle performance, and serum and muscle creatine levels.” Journal of the International Society of Sports Nutrition, 2009; 6: 6. https://doi.org/10.1186/1550-2783-6-6. Creatine Hydrochloride (HCl): Solubility Claims Creatine hydrochloride represents one of the most heavily marketed alternatives to monohydrate, with claims of superior solubility, enhanced absorption, and reduced dosing requirements. Chemical Properties: Creatine HCl binds creatine to hydrochloric acid, creating a salt form with dramatically improved water solubility (approximately 38 times more soluble than monohydrate). This enhanced solubility forms the basis for marketing claims about improved bioavailability63Gufford, B.T., et al. “Physicochemical characterization of creatine N-methylguanidinium salts.” Journal of Dietary Supplements, 2010; 7(3): 240-252. https://doi.org/10.3109/19390211.2010.508034. Scientific Evidence: Direct comparison studies between creatine HCl and monohydrate reveal: A key study by Jagim et al. compared creatine HCl (750mg daily) to creatine monohydrate (3g daily) over 28 days, finding equivalent effects on body composition, strength, and power despite the 4-fold dose difference claimed by marketers. However, when doses were equated for actual creatine content, no differences emerged64Jagim, A.R., et al. “A buffered form of creatine does not promote greater changes in muscle creatine content, body composition, or training adaptations than creatine monohydrate.” Journal of the International Society of Sports Nutrition, 2012; 9(1): 43. https://doi.org/10.1186/1550-2783-9-43. Consumer Implications: Buffered Creatine (Kre-Alkalyn): pH Stability Claims Buffered creatine products claim enhanced stability through alkaline pH buffering, theoretically preventing conversion to creatinine and improving effectiveness. Theoretical Rationale: Creatine spontaneously converts to creatinine (a metabolic waste product) in acidic conditions, including stomach acid. Buffered formulations claim to prevent this conversion, theoretically delivering more intact creatine to muscle tissue65Child, R., & Tallon, M.J. “Creatine ethyl ester rapidly degrades to creatinine in stomach acid.” Biochemical and Biophysical Research Communications, 2007; 364(3): 709-711. https://doi.org/10.1016/j.bbrc.2007.10.082. Research Findings: Controlled studies examining buffered creatine demonstrate: The definitive study by Jagim et al. found no differences between buffered creatine and monohydrate in 36 resistance-trained males over 28 days of supplementation, despite the buffered form costing significantly more66Jagim, A.R., et al. “The acute effects of multi-ingredient pre-workout ingestion on strength performance, lower body power, and anaerobic capacity.” Journal of the International Society of Sports Nutrition, 2013; 10(1): 11. https://doi.org/10.1186/1550-2783-10-11. Creatine Ethyl Ester: Absorption Enhancement Failure Creatine ethyl ester was developed based on the hypothesis that esterification would enhance lipophilicity and improve cellular uptake by bypassing the creatine transporter system. Mechanistic Hypothesis: The ethyl ester modification was intended to: Research Reality: Multiple studies have demonstrated that creatine ethyl ester actually performs worse than monohydrate: Spillane et al. found that creatine ethyl ester supplementation resulted in significantly lower muscle creatine increases compared to monohydrate, with much of the supplement being converted to creatinine and excreted in urine67Spillane, M., et al. “The effects of creatine ethyl ester supplementation combined with heavy resistance training on body composition, muscle performance, and serum and muscle creatine levels.” Journal of the International Society of Sports Nutrition, 2009; 6: 6. https://doi.org/10.1186/1550-2783-6-6. Creatine Nitrate: Nitric Oxide Synergy Claims Creatine nitrate combines creatine with nitrate groups, claiming enhanced performance through dual creatine and nitric oxide pathways. Marketing Claims: Scientific Assessment: Limited research on creatine nitrate reveals: Micronized Creatine: Particle Size Modifications Micronized creatine involves reducing particle size to enhance dissolution and potentially improve absorption characteristics. Technical Process: Micronization reduces particle size from approximately 200-500 microns to 20-200 microns, increasing surface area and potentially improving dissolution rate in liquids68Jäger, R., et al. “The effect of Russian Tarragon (Artemisia dracunculus L.) on the plasma creatine concentration with creatine monohydrate supplementation.” Journal of the International Society of Sports Nutrition, 2008; 5: 8. https://doi.org/10.1186/1550-2783-5-8. Practical Benefits: Efficacy Considerations: Third-Party Testing and Certification The unregulated nature of dietary supplements necessitates careful product selection based on independent quality verification rather than marketing claims alone69Maughan, R.J. “Contamination of dietary supplements and positive drug tests in sport.” Journal of Sports Sciences, 2005; 23(9): 883-889. https://doi.org/10.1080/02640410400023258. Key Certification Programs: Testing Parameters: Quality testing should verify: Red Flags in Product Selection: Cost-Effectiveness Analysis Price Comparison Framework: Effective cost comparison requires evaluating price per gram of actual creatine content rather than total product price, as different forms contain varying concentrations of active compound70Kreider, R.B., & Jung, Y.P. “Creatine supplementation in exercise, sport, and medicine.” Journal of Exercise Nutrition & Biochemistry, 2011; 15(2): 53-69. https://doi.org/10.5717/jenb.2011.15.2.53. Typical Cost Ranges (per gram of creatine content): Value Assessment Criteria: Bulk Purchasing Considerations: The discovery that brain tissue contains the second-highest creatine concentrations in the human body, combined with growing understanding of neuroenergetics in cognitive function, has opened entirely new research domains for creatine supplementation beyond athletic applications71Brosnan, J.T., & Brosnan, M.E. “Creatine: endogenous metabolite, dietary, and therapeutic supplement.” Annual Review of Nutrition, 2007; 27: 241-261. https://doi.org/10.1146/annurev.nutr.27.061406.093621. Neuroenergetics and Cognitive Function The brain’s extraordinary energy demands—consuming approximately 20% of total body energy despite representing only 2% of body weight—require sophisticated energy buffering systems. The creatine-phosphocreatine system serves critical roles in neural energy metabolism, particularly in high-energy processes such as neurotransmitter synthesis, synaptic transmission, and ion pump maintenance72Wallimann, T., et al. “Some new aspects of creatine kinase (CK): compartmentation, structure, function and regulation for cellular and mitochondrial bioenergetics and physiology.” Biofactors, 1998; 8(3-4): 229-234. https://doi.org/10.1002/biof.5520080310. Regional Brain Creatine Distribution: Neuroimaging studies using magnetic resonance spectroscopy reveal distinct patterns of creatine distribution across brain regions: These distribution patterns correlate with regional metabolic activity and help predict which cognitive functions might benefit most from creatine supplementation73Dechent, P., et al. “Increase of total creatine in human brain after oral supplementation of creatine-monohydrate.” American Journal of Physiology, 1999; 277(3): R698-R704. https://doi.org/10.1152/ajpregu.1999.277.3.R698. Cognitive Performance Research Systematic reviews and meta-analyses of cognitive performance studies reveal consistent patterns of benefit, particularly under conditions of metabolic stress, sleep deprivation, or aging74Avgerinos, K.I., et al. “Effects of creatine supplementation on cognitive function of healthy individuals: A systematic review of randomized controlled trials.” Experimental Gerontology, 2018; 108: 166-173. https://doi.org/10.1016/j.exger.2018.04.013. Memory Enhancement: Multiple studies demonstrate improvements in working memory, short-term memory, and long-term memory consolidation with creatine supplementation. The mechanisms likely involve enhanced energy availability for memory-related neural processes and improved neurotransmitter synthesis75Rae, C., et al. “Oral creatine monohydrate supplementation improves brain performance: a double-blind, placebo-controlled, cross-over trial.” Proceedings of the Royal Society B, 2003; 270(1529): 2147-2150. https://doi.org/10.1098/rspb.2003.2492. Key findings include: Stress and Fatigue Resistance: Perhaps the most robust cognitive benefits occur under conditions of mental stress, sleep deprivation, or cognitive fatigue. These scenarios create energy deficits that creatine supplementation can help offset76McMorris, T., et al. “Effect of creatine supplementation and sleep deprivation, with mild exercise, on cognitive and psychomotor performance, mood state, and plasma concentrations of catecholamines and cortisol.” Psychopharmacology, 2006; 185(1): 93-103. https://doi.org/10.1007/s00213-005-0269-z. Research in sleep-deprived individuals shows: Age-Related Cognitive Decline Aging involves multiple changes that could theoretically benefit from creatine supplementation: declining brain creatine levels, reduced mitochondrial function, and increased oxidative stress77Beal, M.F. “Neuroprotective effects of creatine.” Amino Acids, 2011; 40(5): 1305-1313. https://doi.org/10.1007/s00726-011-0851-0. Older Adult Research: Studies in healthy older adults demonstrate: The magnitude of cognitive benefits appears greater in older adults compared to young healthy individuals, suggesting that age-related energy deficits may create greater opportunity for improvement78McMorris, T., et al. “Creatine supplementation and cognitive performance in elderly individuals.” Neuropsychology, Development, and Cognition. Section B, Aging, Neuropsychology and Cognition, 2007; 14(5): 517-528. https://doi.org/10.1080/13825580600788100. Vegetarian Population Benefits: Vegetarians show particularly pronounced cognitive benefits from creatine supplementation, likely reflecting lower baseline brain creatine levels due to absent dietary creatine intake79Benton, D., & Donohoe, R. “The influence of creatine supplementation on the cognitive functioning of vegetarians and omnivores.” British Journal of Nutrition, 2011; 105(7): 1100-1105. https://doi.org/10.1017/S0007114510004733. Cognitive improvements in vegetarians include: The role of bioenergetic dysfunction in neurological diseases has prompted investigation of creatine as a potential therapeutic agent for conditions characterized by impaired cellular energy metabolism80Klopstock, T., et al. “A placebo-controlled crossover trial of creatine in mitochondrial diseases.” Neurology, 2000; 55(11): 1748-1751. https://doi.org/10.1212/WNL.55.11.1748. Parkinson’s Disease Research Parkinson’s disease involves progressive degeneration of dopaminergic neurons in the substantia nigra, with emerging evidence suggesting that mitochondrial dysfunction and energy deficits contribute to disease progression81Matthews, R.T., et al. “Creatine and cyclocreatine attenuate MPTP neurotoxicity.” Experimental Neurology, 1999; 157(1): 142-149. https://doi.org/10.1006/exnr.1999.7049. Preclinical Evidence: Animal studies demonstrate that creatine supplementation can: Clinical Trial Results: Human studies in Parkinson’s disease have produced mixed but generally promising results: The largest clinical trial (NET-PD LS1) found trends toward benefit that did not reach statistical significance, but post-hoc analyses suggested benefits in specific subgroups, leading to ongoing research in early-stage disease82NINDS NET-PD Investigators. “A randomized, double-blind, futility clinical trial of creatine and minocycline in early Parkinson disease.” Neurology, 2006; 66(5): 664-671. https://doi.org/10.1212/01.wnl.0000201252.57661.e1. Huntington’s Disease Investigation Huntington’s disease represents an inherited neurodegenerative condition characterized by progressive motor, cognitive, and psychiatric symptoms. Energy metabolism dysfunction appears early in disease progression, making creatine a logical therapeutic target83Hersch, S.M., et al. “Creatine in Huntington disease is safe, tolerable, bioavailable in brain and reduces serum 8OH2’dG.” Neurology, 2006; 66(2): 250-252. https://doi.org/10.1212/01.wnl.0000194318.74946.b6. Mechanistic Rationale: Research Progress: Amyotrophic Lateral Sclerosis (ALS) Research ALS involves progressive degeneration of motor neurons, with evidence suggesting that energy metabolism dysfunction contributes to disease progression. Creatine research in ALS has produced mixed results but continues to generate interest84Klivenyi, P., et al. “Neuroprotective effects of creatine in a transgenic animal model of amyotrophic lateral sclerosis.” Nature Medicine, 1999; 5(3): 347-350. https://doi.org/10.1038/6568. Theoretical Benefits: Clinical Trial Outcomes: Results have been inconsistent, with some studies showing modest benefits and others finding no significant effects. The heterogeneity of ALS may require more targeted approaches based on disease subtype or progression stage85Groeneveld, G.J., et al. “A randomized sequential trial of creatine in amyotrophic lateral sclerosis.” Annals of Neurology, 2003; 53(4): 437-445. https://doi.org/10.1002/ana.10554. Emerging research suggests that creatine supplementation may offer therapeutic benefits for mood disorders, particularly depression, through mechanisms involving brain energy metabolism and neurotransmitter systems86Roitman, S., et al. “Creatine monohydrate in resistant depression: a preliminary study.” Bipolar Disorders, 2007; 9(7): 754-758. https://doi.org/10.1111/j.1399-5618.2007.00532.x. Neurobiological Mechanisms Depression involves complex alterations in brain energy metabolism, neurotransmitter function, and neural plasticity. Several mechanisms could theoretically explain creatine’s potential antidepressant effects: Energy Metabolism: Neurotransmitter Systems: Clinical Research Evidence The most compelling evidence comes from studies examining creatine as an adjunctive treatment for depression, particularly in women87Lyoo, I.K., et al. “A randomized, double-blind placebo-controlled trial of oral creatine monohydrate augmentation for enhanced response to a selective serotonin reuptake inhibitor in women with major depressive disorder.” American Journal of Psychiatry, 2012; 169(9): 937-945. https://doi.org/10.1176/appi.ajp.2012.12010009. Landmark Study by Lyoo et al.: This randomized, double-blind, placebo-controlled trial examined creatine supplementation (5g daily) as an adjunct to SSRI treatment in women with major depressive disorder. Key findings included: Gender Differences: Several studies suggest that women may show greater antidepressant responses to creatine supplementation, possibly related to: Bipolar Disorder Research: Preliminary studies in bipolar disorder suggest potential benefits for both depressive and manic symptoms: Age-related muscle loss (sarcopenia) affects approximately 10% of adults over 60 and up to 50% of those over 80, contributing significantly to disability, falls, fractures, and loss of independence. Creatine supplementation combined with resistance exercise represents a promising intervention for preserving muscle mass and function during aging88Candow, D.G., & Chilibeck, P.D. “Creatine supplementation and aging musculoskeletal health.” Endocrine, 2008; 33(3): 245-254. https://doi.org/10.1007/s12020-008-9070-4. Age-Related Changes in Muscle Creatine Systems Aging involves multiple changes that could impair muscle creatine systems and potentially benefit from supplementation: Muscle Composition Changes: Metabolic Alterations: These age-related changes create a theoretical framework for creatine supplementation benefits, as the supplement could help overcome energy deficits and enhance the anabolic response to resistance exercise89Gotshalk, L.A., et al. “Creatine supplementation improves muscular performance in older women.” European Journal of Applied Physiology, 2008; 102(2): 223-231. https://doi.org/10.1007/s00421-007-0580-y. Research in Older Adult Populations Systematic reviews and meta-analyses of creatine supplementation in older adults demonstrate consistent benefits when combined with resistance training, with effect sizes often exceeding those observed in younger populations90Devries, M.C., & Phillips, S.M. “Creatine supplementation during resistance training in older adults-a meta-analysis.” Medicine & Science in Sports & Exercise, 2014; 46(6): 1194-1203. https://doi.org/10.1249/MSS.0000000000000220. Strength and Power Improvements: Studies in older adults (age 65-80) show: Muscle Mass Preservation: Long-term studies demonstrate that creatine supplementation can: Bone Health Interactions: Emerging research suggests potential benefits for bone health in older adults: Specialized Protocols for Aging Populations Older adults may benefit from modified creatine supplementation protocols that account for age-related changes in absorption, metabolism, and exercise capacity91Chilibeck, P.D., et al. “Creatine monohydrate supplementation does not prevent muscle loss or affect markers of bone turnover in older males during 10 days of bed rest.” Journal of Nutrition, Health & Aging, 2008; 12(7): 438-444. https://doi.org/10.1007/BF02982674. Dosing Modifications: Exercise Integration: Frailty Prevention and Treatment Frailty represents a clinical syndrome characterized by decreased reserve and resistance to stressors, resulting from cumulative decline across multiple physiological systems. Creatine supplementation shows promise as an intervention for both preventing and treating frailty92Gualano, B., et al. “Creatine supplementation in the aging population: effects on skeletal muscle, bone and brain.” Amino Acids, 2014; 46(8): 1831-1838. https://doi.org/10.1007/s00726-014-1775-5. Frailty Characteristics Potentially Responsive to Creatine: Preliminary Research Results: Small studies in frail older adults suggest: The relationship between creatine supplementation and glucose metabolism represents an emerging area of research with potential implications for diabetes prevention and management93Gualano, B., et al. “Does creatine supplementation affect glucose homeostasis?” Medicine & Science in Sports & Exercise, 2008; 40(11): 1905-1912. https://doi.org/10.1249/MSS.0b013e318181463a. Mechanisms of Glucose Metabolism Effects Several mechanisms could theoretically explain creatine’s effects on glucose homeostasis: Muscle Glucose Uptake: Cellular Energy Status: Research Findings and Clinical Implications Studies examining glucose metabolism effects have produced mixed results, highlighting the complexity of creatine’s metabolic interactions94Salomons, G.S., et al. “Creatine deficiency in the brain: a new, treatable inborn error of metabolism.” Pediatric Research, 2001; 49(3): 410-418. https://doi.org/10.1203/00006450-200103000-00016. Positive Effects Observed: Neutral or Negative Effects: Clinical Recommendations: Type 2 Diabetes Research Limited research in individuals with type 2 diabetes suggests potential benefits, but results remain preliminary and require further investigation 95Earnest, C.P., et al. “The effect of creatine monohydrate ingestion on anaerobic power indices, muscular strength and body composition.” Acta Physiologica Scandinavica, 1995; 153(2): 207-209. https://doi.org/10.1111/j.1748-1716.1995.tb09854.x. Potential Benefits: Safety Considerations: The strategic implementation of creatine supplementation within periodized training programs requires understanding of how the supplement’s benefits align with different training phases and competitive demands96Kreider, R.B. “Effects of creatine supplementation on performance and training adaptations.” Molecular and Cellular Biochemistry, 2003; 244(1-2): 89-94. https://doi.org/10.1023/A:1022465203458. Macrocycle Integration Off-Season/Base Building Phase: During periods of high training volume and strength development focus: Pre-Competition Phase: As training shifts toward sport-specific and high-intensity work: Competition Phase: During competitive seasons with irregular training patterns: Recovery/Transition Phase: Between competitive seasons or during planned breaks: Sport-Specific Applications Power and Strength Sports (Weightlifting, Powerlifting, Throwing): Team Sports (Soccer, Basketball, Hockey): Combat Sports (Boxing, MMA, Wrestling): Endurance Sports (Cycling, Running, Triathlon): Seasonal Timing Strategies Loading Phase Timing: Strategic implementation of loading protocols around key training or competition periods: Maintenance Adjustments: Modify maintenance dosing based on training and competition demands: Creatine’s excellent safety profile and well-understood mechanisms make it compatible with most other supplements commonly used by athletes and fitness enthusiasts. However, understanding potential interactions and synergies can optimize overall supplementation strategies97Kerksick, C.M., et al. “International society of sports nutrition position stand: nutrient timing.” Journal of the International Society of Sports Nutrition, 2017; 14: 33. https://doi.org/10.1186/s12970-017-0189-4. Protein Supplementation Synergies The combination of creatine and protein supplementation represents one of the most researched and practically beneficial supplement combinations for athletes and individuals engaged in resistance training98Burke, D.G., et al. “The effect of whey protein supplementation with and without creatine monohydrate combined with resistance training on lean tissue mass and muscle strength.” International Journal of Sport Nutrition and Exercise Metabolism, 2001; 11(3): 349-364. https://doi.org/10.1123/ijsnem.11.3.349. Mechanistic Synergies: Practical Implementation: Research Support: Studies combining creatine and protein supplementation consistently show: Beta-Alanine Combinations Beta-alanine and creatine target different energy systems and fatigue mechanisms, creating potential for complementary benefits during high-intensity exercise99Hoffman, J., et al. “Effect of creatine and beta-alanine supplementation on performance and endocrine responses in strength/power athletes.” International Journal of Sport Nutrition and Exercise Metabolism, 2006; 16(4): 430-446. https://doi.org/10.1123/ijsnem.16.4.430. Complementary Mechanisms: Implementation Strategies: Performance Benefits: Research combining both supplements demonstrates: Caffeine Interaction Considerations The relationship between creatine and caffeine remains one of the most debated topics in sports nutrition, with conflicting research results and ongoing theoretical discussions100Vandenberghe, K., et al. “Caffeine counteracts the ergogenic action of muscle creatine loading.” Journal of Applied Physiology, 1996; 80(2): 452-457. https://doi.org/10.1152/jappl.1996.80.2.452. Historical Controversy: Early research by Vandenberghe et al. suggested that caffeine might blunt creatine’s ergogenic effects, leading to recommendations for avoiding concurrent use. However, subsequent research has provided a more nuanced understanding101Trexler, E.T., et al. “Effects of coffee and caffeine anhydrous intake during creatine loading.” Journal of Strength and Conditioning Research, 2016; 30(5): 1438-1446. https://doi.org/10.1519/JSC.0000000000001223. Current Understanding: Practical Recommendations: Carbohydrate Supplementation Enhancement Carbohydrate co-ingestion with creatine enhances muscle uptake through insulin-mediated improvements in transporter activity, making this combination particularly valuable during loading phases102Steenge, G.R., et al. “Protein- and carbohydrate-induced augmentation of whole body creatine retention in humans.” Journal of Applied Physiology, 2000; 89(3): 1165-1171. https://doi.org/10.1152/jappl.2000.89.3.1165. Optimal Carbohydrate Protocols: Alternative Approaches: Female Athletes and Gender-Specific Factors While the majority of creatine research has been conducted in male populations, growing evidence suggests similar benefits in female athletes with some unique considerations103Kambis, K.W., & Pizzedaz, S.K. “Short-term creatine supplementation improves maximum quadriceps contraction in women.” International Journal of Sport Nutrition and Exercise Metabolism, 2003; 13(1): 87-96. https://doi.org/10.1123/ijsnem.13.1.87. Physiological Differences: Research Findings in Women: Studies in female athletes demonstrate: Menstrual Cycle Considerations: Pregnancy and Lactation: Adolescent Athletes The use of creatine supplementation in adolescent athletes requires careful consideration of developmental factors, safety concerns, and appropriate supervision104Unnithan, V.B., et al. “Is there a physiologic basis for creatine use in children and adolescents?” Journal of Strength and Conditioning Research, 2001; 15(4): 524-528.. Developmental Considerations: Safety Evidence: Research in adolescent populations shows: Implementation Guidelines: Conservative Protocols for Adolescents: The supplement industry continues developing innovative approaches to creatine delivery, though most innovations require rigorous scientific validation before clinical adoption105Kreider, R.B., et al. “ISSN exercise & sports nutrition review update: research & recommendations.” Journal of the International Society of Sports Nutrition, 2018; 15(1): 38. https://doi.org/10.1186/s12970-018-0242-y. Liposomal Encapsulation Technology Liposomal delivery systems encapsulate creatine within phospholipid vesicles, theoretically enhancing cellular uptake and bioavailability while reducing gastrointestinal side effects. Theoretical Advantages: Research Status: Nanotechnology Applications Nanotechnology approaches to creatine delivery involve reducing particle size to nanometer dimensions, potentially enhancing dissolution and absorption characteristics. Proposed Mechanisms: Current Research Status: Sustained-Release Formulations Time-release creatine formulations aim to provide steady creatine levels throughout the day, potentially improving muscle uptake efficiency and reducing side effects. Design Principles: Research Considerations: Advances in genetic testing, biomarker analysis, and individual response profiling are enabling more personalized approaches to creatine supplementation106Hubal, M.J., et al. “Variability in muscle size and strength gain after unilateral resistance training.” Medicine & Science in Sports & Exercise, 2005; 37(6): 964-972. https://doi.org/10.1249/01.MSS.0000170469.90461.5F. Genetic Testing Applications Commercial genetic testing panels increasingly include polymorphisms relevant to creatine metabolism, transport, and response prediction. Clinically Relevant Polymorphisms: Implementation Strategies: Limitations and Considerations: Biomarker-Guided Supplementation Development of accessible biomarkers for creatine status and supplementation response could enable more precise dosing and monitoring protocols. Potential Biomarkers: Monitoring Applications: Artificial Intelligence and Machine Learning Advanced analytical approaches may enable better prediction of individual creatine responses based on multiple factors including genetics, training history, body composition, and performance metrics107Bamman, M.M., et al. “Cluster analysis tests the importance of myogenic gene expression during myofiber hypertrophy in humans.” Journal of Applied Physiology, 2007; 102(6): 2232-2239. https://doi.org/10.1152/japplphysiol.00024.2007. Predictive Modeling Applications: Data Integration Challenges: Growing understanding of creatine’s mechanisms beyond energy metabolism is driving research into novel therapeutic applications across multiple medical specialties108Wyss, M., & Schulze, A. “Health implications of creatine: can oral creatine supplementation protect against neurological and atherosclerotic disease?” Neuroscience, 2002; 112(2): 243-260. https://doi.org/10.1016/S0306-4522(02)00088-X. Cardiovascular Disease Applications Heart failure and other cardiovascular conditions involve energy metabolism dysfunction that could theoretically benefit from creatine supplementation. Mechanistic Rationale: Current Research Status: Cancer-Related Applications Cancer treatment-related fatigue and muscle wasting represent potential applications for creatine supplementation, though research remains early-stage109Norman, K., et al. “Hand grip strength: outcome predictor and marker of nutritional status.” Clinical Nutrition, 2011; 30(2): 135-142. https://doi.org/10.1016/j.clnu.2010.09.010. Theoretical Benefits: Research Challenges: Metabolic Syndrome and Diabetes The growing epidemic of metabolic syndrome and type 2 diabetes has prompted investigation of creatine’s potential therapeutic role in metabolic health110Gualano, B., et al. “Creatine in type 2 diabetes: a randomized, double-blind, placebo-controlled trial.” Medicine & Science in Sports & Exercise, 2011; 43(5): 770-778. https://doi.org/10.1249/MSS.0b013e3181fcee7d. Potential Mechanisms: Research Priorities: The creatine supplement industry continues evolving toward higher quality standards and better regulatory oversight, driven by consumer demand and scientific advancement111111 Maughan, R.J., et al. “IOC consensus statement: dietary supplements and the high-performance athlete.” British Journal of Sports Medicine, 2018; 52(7): 439-455. https://doi.org/10.1136/bjsports-2018-099027. Enhanced Testing Standards Third-party testing organizations are implementing more comprehensive testing protocols that go beyond basic purity and potency verification. Advanced Testing Parameters: Emerging Certification Programs: International Harmonization Efforts Global efforts are underway to harmonize creatine supplement standards across different regulatory jurisdictions. Standardization Goals: Challenges and Progress: Digital Innovation in Quality Assurance Technology integration is enabling new approaches to supplement quality verification and consumer protection. Blockchain Applications: Smart Packaging Technologies: Creatine monohydrate stands as the most extensively researched and scientifically validated performance supplement in human history, with over 2,500 peer-reviewed studies establishing its safety and efficacy across multiple domains of human performance and health. This unprecedented research foundation, spanning four decades of rigorous scientific investigation, provides unparalleled confidence in creatine’s risk-benefit profile and practical applications. The convergence of robust mechanistic understanding, consistent clinical outcomes, excellent safety profile, and practical accessibility makes creatine supplementation an evidence-based choice for diverse populations seeking to optimize training adaptations, enhance performance outcomes, and potentially improve various aspects of health and cognitive function. From elite athletes pursuing marginal performance gains that determine competitive success to older adults seeking to maintain muscle mass and functional capacity, creatine offers documented benefits supported by the highest levels of scientific evidence. The key to successful creatine implementation lies in understanding the complex interplay of genetic, physiological, and environmental factors that influence individual response patterns. While not all users will experience dramatic improvements, the potential benefits far outweigh the minimal risks and costs associated with proper supplementation using pharmaceutical-grade creatine monohydrate. As research continues expanding into therapeutic applications beyond athletic performance—including cognitive enhancement, neuroprotection, aging interventions, and metabolic health—creatine’s relevance may extend to broader populations seeking evidence-based approaches to health optimization. However, the foundation of performance benefits established through decades of research in athletic populations provides the strongest current rationale for supplementation among active individuals. For those considering creatine supplementation, starting with pharmaceutical-grade creatine monohydrate using established dosing protocols represents the most evidence-based approach. The extensive research supporting creatine’s benefits, combined with its excellent safety profile and cost-effectiveness, ensures that this supplement will continue serving as a cornerstone of sports nutrition and performance optimization for decades to come. The future of creatine research lies not in questioning its fundamental efficacy—which has been conclusively established—but in optimizing individual applications through personalized protocols, expanding therapeutic applications, and continuing to explore the full potential of this remarkable compound for human health and performance enhancement. Most supplement advice ignores timing, interactions, and dose-response curves. Smart Stack Builder doesn't. Get a personalized daily schedule with interaction flags and dosage guidance, built on the same evidence base as this article.
Advanced Timing and Co-ingestion Strategies
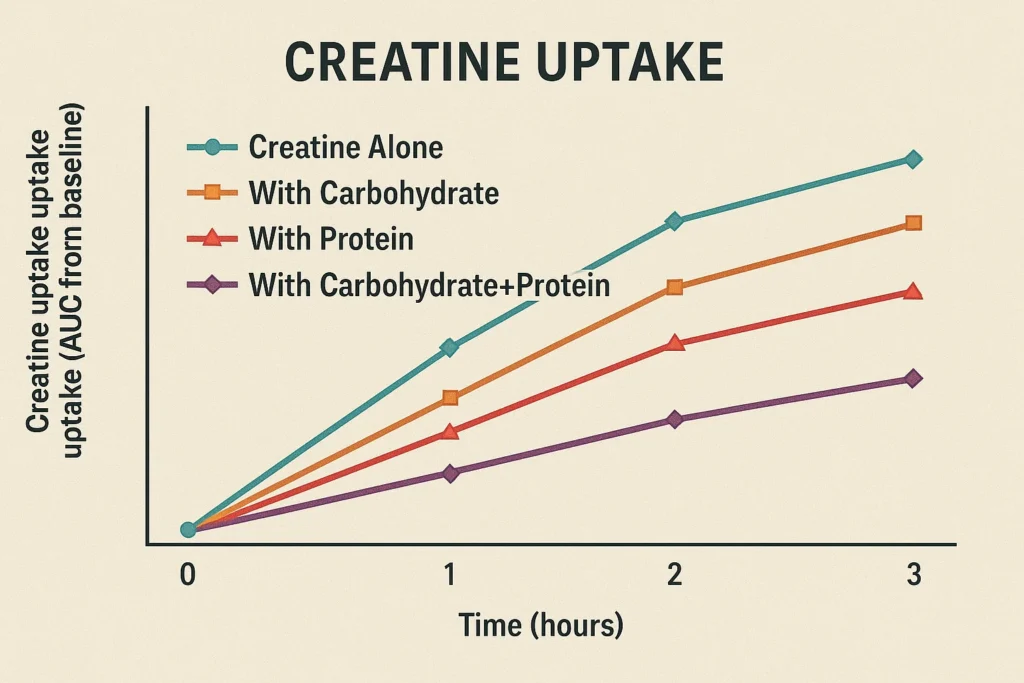
Specialized Protocols for Specific Populations
Comprehensive Safety Analysis and Long-Term Health Effects
Short-Term Safety Profile and Adverse Event Management
Long-Term Safety and Organ System Effects
Drug Interactions and Contraindications
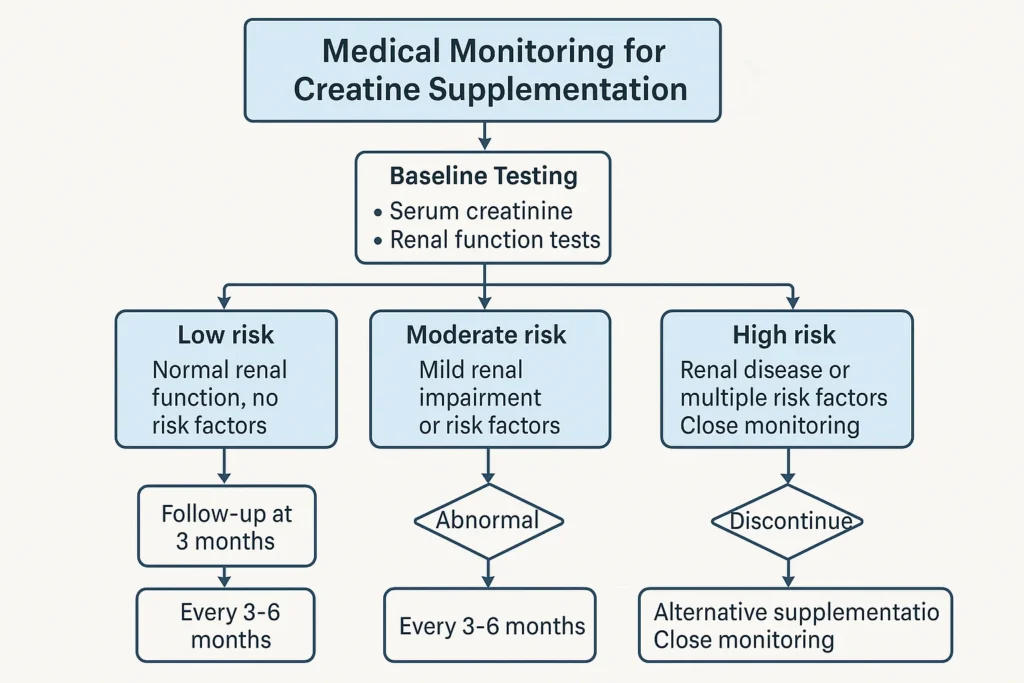
Individual Variation and Response Optimization
Genetic Factors Influencing Creatine Response
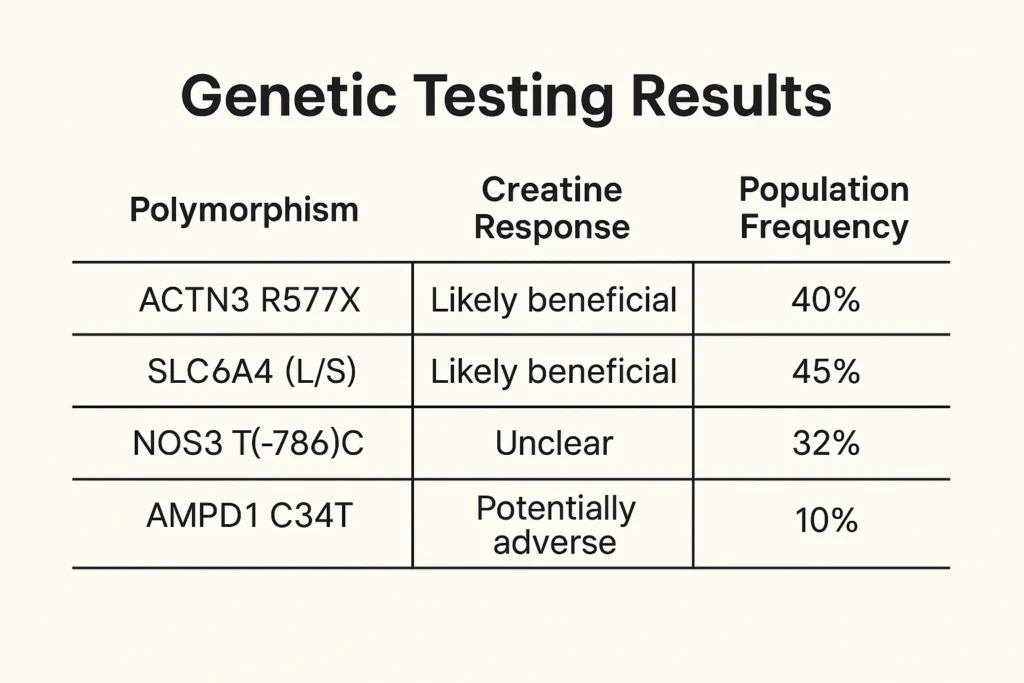
Physiological Factors Affecting Individual Response
Dietary and Lifestyle Factors
Response Monitoring and Assessment Strategies
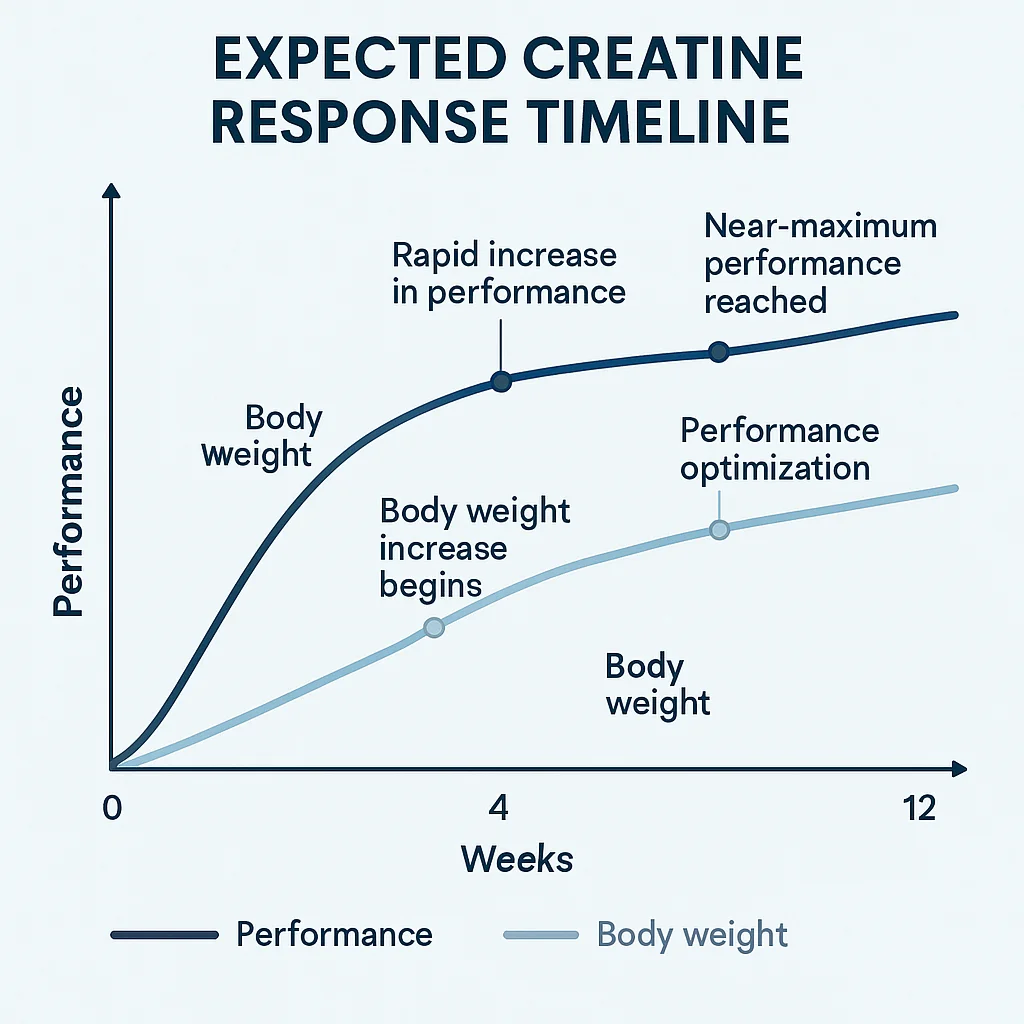
Creatine Forms: Scientific Comparison and Consumer Guidance
Creatine Monohydrate: The Research Gold Standard
Alternative Creatine Forms: Marketing vs. Science
Quality Assessment and Product Selection
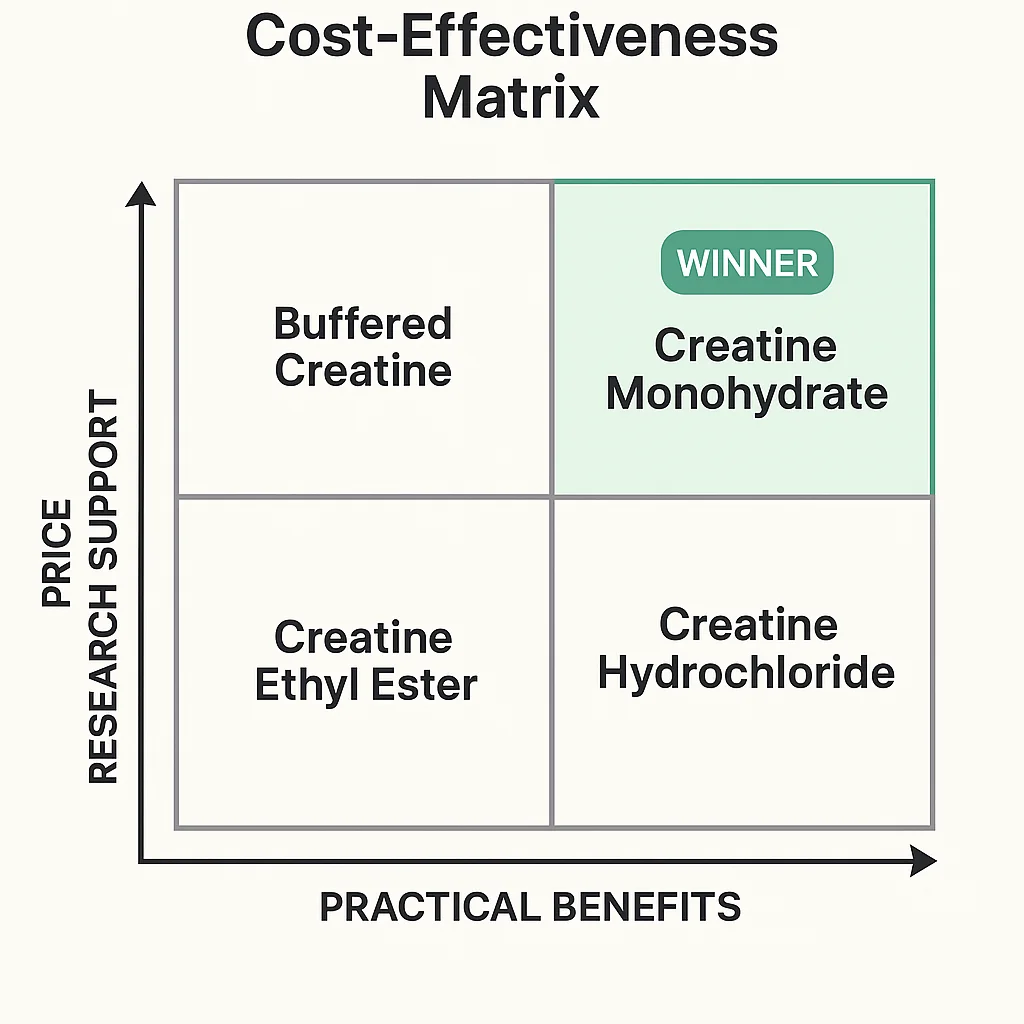
Emerging Therapeutic Applications
Cognitive Enhancement and Neuroprotection
Neurological and Neurodegenerative Disease Applications
Depression and Mood Disorders
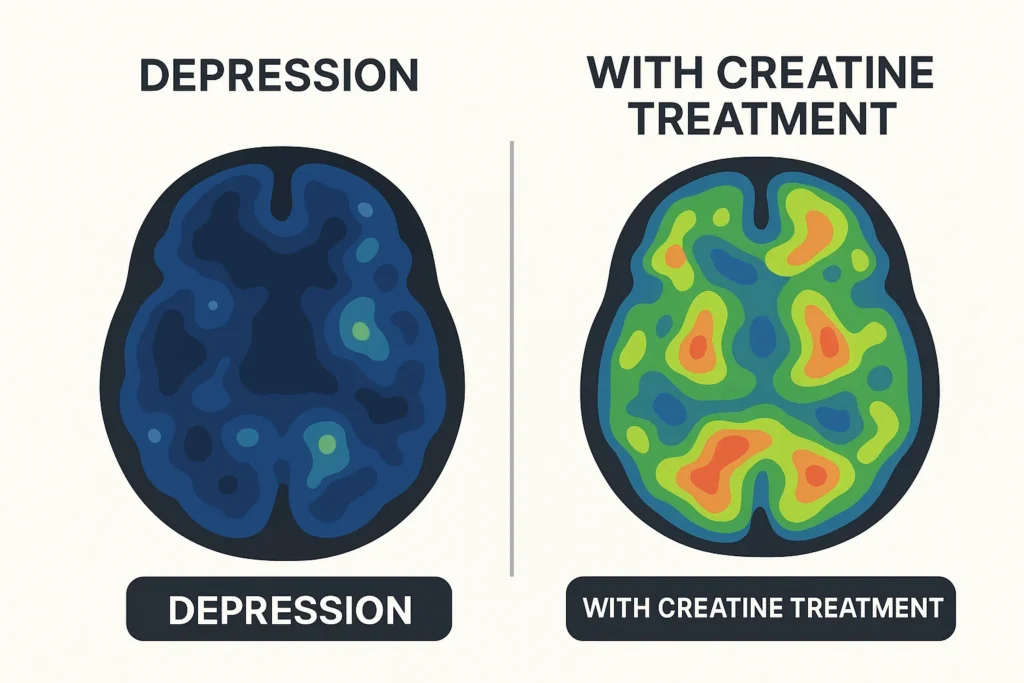
Aging, Sarcopenia, and Muscle Health
Metabolic Health and Glucose Regulation
Advanced Implementation Strategies
Periodization and Athletic Applications
Integration with Other Supplements
Special Population Considerations
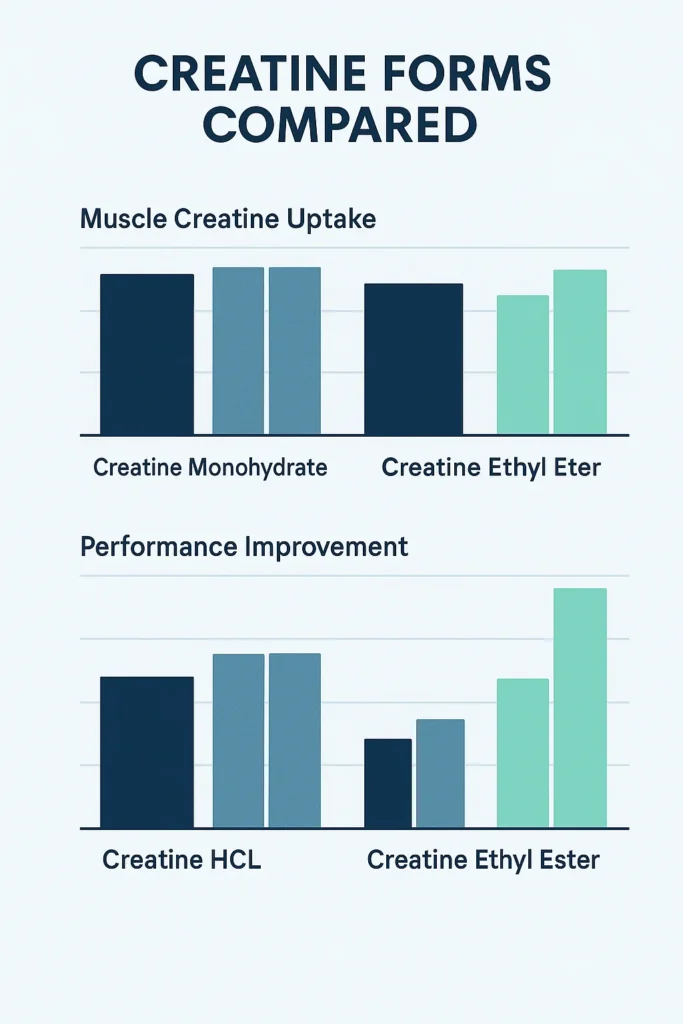
Future Directions and Emerging Research
Novel Delivery Systems and Formulations
Precision Nutrition and Personalized Protocols
Therapeutic Applications Expansion
Regulatory and Quality Assurance Evolution
Comprehensive Conclusion
Generate Your Stack. Avoid Conflicts. Optimize Absorption.
References
This article is part of our Supplements hub: A science-backed collection of ingredient research, clinical dosage reviews, and optimized stack insights.